

SISE - Standardisation in Surgical Education
SISE is an innovative, structured approach to surgical training that places patient safety at its core. By ensuring that the initial learning curve takes place entirely in a simulation-based environment, SISE allows surgeons to develop and refine their skills without exposing patients to unnecessary risk.
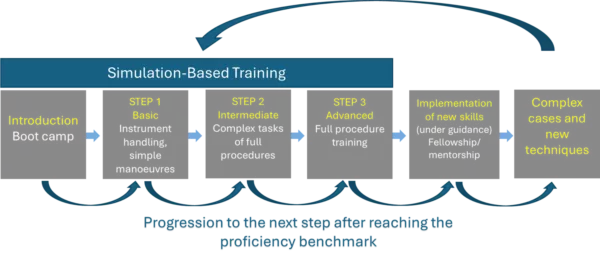
Through a progressive, proficiency-based pathway, from basic techniques to full procedural training, surgeons advance only after meeting clearly defined benchmarks. This structured methodology not only ensures consistent skill acquisition, but also optimizes training efficiency by focusing on targeted practice, objective assessment, and stepwise progression.
What we do
- Provide international guidance on surgical training, to allow surgeons achieve competence by following pre-defined, standardised pathways
- Wide-spread SISE standards globally with courses, events and dedicated study programmes, to raise the level of urological care throughout Europe and beyond
- Implement courses locally according to international standards
- Create an international network of certified trainers and training centers
- Collect data to improve the educational system through certification and new quality benchmarks
- Contribute to the determination of European urological health care policies
History
The SISE programme was founded in 2019 by The European School of Urology (ESU) who delivers the education needs of urologists on behalf of the EAU Education Office. The ESU succesfully applied for an ERASMUS+ grant in collaboration with 6 leading institutions in the field of minimally-invasive surgery (MIS) field. These 6 leading institutions are Academisch Medisch Centrum (NL), SLK-Kliniken Heilbronn (DE), Institutul Oncologic Cluj-Napoca (RO), Uniwersytet Mikołaja Kopernika w Toruniu (PL), Univerzita Karlova (CZ) and Panepistimio Patron (GR).
Addressing the need for modern urological training, multiple methodologies have been developed in the last 20 years, starting from the original “learning-by-watching” dogma. This resulted in the production of a large pool of surgeons around Europe, who reached their professional proficiency with individualized modalities. However, these process was not following a planned pathway and was lacking measurability and replicability between different countries. In EAU we believe that between the most important goals of a scientific society, is wide-spreading education to guarantee the highest standards in patient safety. Therefore, in 2011 the European School of Urology (ESU) started with the development of standardized training programs for urological surgery. These research procedures were further supported and optimized since September 2013, by the newly instituted “ESU training research group”, which coordinated development and testing of new protocols in collaboration with the EAU section offices. In 2019 the ESU training research group successfully applied for a ERASMUS + grant to kick start the SISE programme.
Founding members
J. Palou, Barcelona (ES)
E. Liatsikos, Patras (GR)
B. Van Cleynenbreugel, Leuven (BE)
A. Gözen, Heilbronn (DE)
B. Somani, Southampton (GB)
D. Veneziano, Reggio Calabria (IT)
K. Ahmed, London (GB)
T. Brouwers, Wijchen (NL)
References
- Satava R, Gallagher A. Next generation of procedural skills curriculum development: Proficiency-based progression. J Heal Spec. 2015;3(4):198. doi:10.4103/1658-600X.166497
- Salmon P, Stanton N, Gibbon A, Jenkins D, Walker G. Cognitive Task Analysis. In: Human Factors Methods and Sports Science. ; 2009. doi:10.1201/9781420072181-c4
- Messick S. Validity of Psychological Assessment. Am Psychol. 1995. doi:10.1037//0003-066X.50.9.741
- Korndorffer JR, Kasten SJ, Downing SM. A call for the utilization of consensus standards in the surgical education literature. Am J Surg. 2010;199(1):99-104. doi:10.1016/j.amjsurg.2009.08.018
- Sweet RM, Hananel D, Lawrenz F. A unified approach to validation, reliability, and education study design for surgical technical skills training. Arch Surg. 2010. doi:10.1001/archsurg.2009.266
- Goldenberg M, Lee JY. Surgical Education, Simulation, and Simulators—Updating the Concept of Validity. Curr Urol Rep. 2018;19(7). doi:10.1007/s11934-018-0799-7
- Satava RM. The future of sugical simulation and surgical robotics. Bull Am Coll Surg. 2007.