
5. DIAGNOSTIC EVALUATION
A comprehensive diagnostic evaluation of urethral stricture disease encompasses clinical history and examination, urinalysis (+/- culture), uroflowmetry and post-void residual (PVR) assessment, radiography and endoscopy.
5.1. Patient history
The purpose of history-taking is to assess symptoms including severity and duration, possible aetiology, prior treatments, complications, associated problems and patient factors that may impact upon surgical outcome.
The clinical presentation of urethral stricture disease is varied. In a retrospective analysis of 611 patients with an endoscopically confirmed diagnosis of urethral stricture, LUTS were the most common presentation (54.3%) followed by acute urinary retention (22.3%), urinary tract infection (UTI) (6.1%) and difficult catheterisation (4.8%) [155]. In a retrospective study of 214 patients who underwent anterior urethroplasty, weak stream was reported as the most common individual LUTS (49%), followed by incomplete emptying (27%) and urinary frequency (20%) [156]. A further retrospective series of 614 patients undergoing anterior urethroplasty found post-void dribble to be present in 73% [157].
Genitourinary pain is a common feature, affecting 22.9–71% of patients [29,155,158]. Pain may be felt in the bladder and/or urethra, is associated with more severe LUTS, is more likely to be felt by younger men, and resolves in most following reconstruction [158]. Other complaints include spraying (9%), visible haematuria (3.1–5%), urethral abscess/necrotising fasciitis (2.3%), urgency (14%) and incontinence (1–4%) [155, 156].
To establish aetiology, an enquiry about a history of pelvic, genital or perineal trauma, prior instrumentation, prior surgeries, irradiation or focal therapies and urethritis should be made. It is important to document prior surgical approaches and date of the most recent intervention (e.g. dilatation), as this may impact upon the timing of radiological evaluation or surgical treatment.
Problems of sexual function are common in patients with urethral stricture disease [159,160] and sexual function may be impacted upon by surgical intervention [161, 162]. Therefore, the status of erectile and ejaculatory function should be established and documented using validated tools.
The performance status of the patient should be determined, as it may influence the choice of treatment (curative or palliative). A past medical history should assess factors that may impact upon tissue healing including diabetes, immunosuppression and smoking. Oral tobacco use or the chewing of betel leaves may increase the risk of morbidity at the harvest site or render oral mucosa too poor for use. Prior harvest of oral mucosa should be noted as alternative sources for tissue transfer [163] or alternative surgical approaches (e.g. perineal urethrostomy [PU]) may need to be considered.
5.2. Physical examination
The abdomen should be examined for the presence of a palpable bladder. The location of any suprapubic tube should be noted to assess its potential utility for antegrade cystoscopy or the placement of a sound (to facilitate repair) [164]. Examination of the genitalia should note the presence of foreskin, the position and size of the meatus, as well as any evidence of scarring suggestive of LS. Preoperative biopsy to confirm LS may be performed if this alters management and is essential if malignancy is suspected [165].
The presence of penile or perineal fistulae should be noted. The urethra should be palpated to assess for induration suggestive of significant fibrosis. In rare cases, a mass may signify a urethral carcinoma. A rectal examination to assess for prostatic pathology, which may be the cause of urinary symptoms, should be undertaken. In patients with posterior urethral stenosis, rectal adherence to the prostate and the mobility of the surrounding tissues should be assessed [166]. The oral cavity should be examined for the suitability of oral mucosa. Measurement of BMI will identify obese individuals who are at greater risk of leg compartment syndrome when placed in the lithotomy position for a prolonged time period [167]. Assessing hip mobility is important when considering an exaggerated lithotomy position, as some patients may have limited hip flexion due to unresolved orthopaedic problems [164].
5.2.1. Further diagnostic evaluation
5.2.1.a. Patient reported outcome measure (PROM)
The first validated urethral stricture surgery PROM (USS-PROM) was reported in 2011[168]. It consists of six LUTS questions derived from the International Consultation on Incontinence Questionnaire Male LUTS (ICIQ- MLUTS) module, a LUTS-specific QoL question, the Peeling voiding chart and the EQ-5D to assess overall health-related QoL (HRQoL). The postoperative questionnaire contains an additional two questions to assess overall patient satisfaction. This PROM has been validated in several other languages (German, Spanish, Italian, Dutch, Turkish, Polish, Japanese) and is increasingly used in research studies, as well as in clinical practice. A further PROM is in development in North America but requires validation [169] (see Section 11).
| Summary of evidence | LE |
| A specific urethral stricture surgery patient reported outcome measure was found to have psychometric validity in the assessment of patient-derived benefit from surgical intervention for urethral stricture disease. | 2a |
| Sexual dysfunction is prevalent in patients with urethral strictures and sexual function can be affected by surgical management of urethral stricture. | 3 |
| Recommendations | Strength rating |
| Use a validated patient reported outcome measure to assess symptom severity and impact upon quality of life in males undergoing surgery for urethral stricture disease. | Strong |
| Use a validated tool to assess sexual function in males undergoing surgery for urethral stricture disease. | Strong |
5.2.1.b. Urinalysis and urine culture
Urinalysis is an essential component of the work-up of patients with LUTS. If infection is suggested, urine culture should be performed to confirm the diagnosis and identify the causative organism and sensitivity to antibiotics. Bacteriuria should be treated prior to surgical intervention to prevent perioperative sepsis [170] (see Chapter 10).
5.2.1.c. Uroflowmetry and post-void residual estimation
A reduced maximum flow rate with a prolonged plateau is characteristic of the constrictive obstruction caused by urethral stricture. However, interpretation of flow patterns is subjective and is not considered a reliable screening tool for the detection of stricture [171]. To overcome this, a statistical model based on uroflowmetry parameters was developed and was found to predict urethral stricture with a sensitivity of 80–81% and a specificity of 77–78% [171]. Uroflowmetry is usually combined with ultrasound (US) estimation of PVR to identify patients with urinary retention who may require emergent bladder drainage. Uroflowmetry parameters can also be used for monitoring patients and in the assessment of treatment response (see Chapter 11).
Urodynamic studies are not indicated in the vast majority of patients with urethral stricture disease. In patients with suspected bladder dysfunction (e.g. severe storage LUTS, history of irradiation or neurological disease), an assessment of bladder function may help surgical decision making and patient counselling. Similarly, when there is concern that flow impairment or increased PVR are due to detrusor underactivity or an acontractile detrusor, a urodynamic study may help predict the likelihood that the patient would need to perform intermittent self-catheterisation (ISC) postoperatively. The only urodynamic parameter found to distinguish a diagnosis of urethral stricture from BPO is urethral closure pressure which is lower in the former due to the constrictive nature of the obstruction (22.07 vs. 28.4cm H2O, p = 0.0039, r = 0.61, BPO vs. stricture) [172].
| Summary of evidence | LE |
| An RCT with more than 12-months follow-up failed to demonstrate a significant reduction in stricture rate using routine urethrotomy prior to TURP. | 1b |
| Recommendation | Strength rating |
| Perform uroflowmetry and estimation of post-void residual in patients with suspected urethral stricture disease. | Strong |
5.2.1.d. Urethrography
Retrograde urethrography (RUG) has been widely used as the investigation of choice for evaluating the stricture presence, location, length and any associated anomalies (e.g. false passages, diverticula) [173].
The reported sensitivity and specificity of RUG in the diagnosis of strictures is 91% and 72%, respectively [174]. The positive predictive value (PPV) was 89%, and the negative predictive value (NPV) was 76% [174]. Most reports suggest that RUG underestimates stricture length [175,176]. Interpretation of RUG findings by urologists were found to be more accurate at predicting urethral stricture location and length as compared to evaluation by an independent physician [177]. However, even amongst urologists, poor inter-rater reliability of stricture length, location and caliber was found [178].
Limitations of RUG include difficulty assessing very distal strictures and assessing the proximal extent of strictures, which are too narrow to permit passage of adequate contrast. Combining a RUG with voiding cystourethrography (VCUG) can allow adequate visualisation of the urethra proximal to the stricture and a more accurate assessment of stricture length in (nearly) obliterative strictures, stenoses and gap in pelvic fracture urethral injury (PFUI) [179, 180]. The position of the proximal urethral end (in relation to the pubic symphysis) in PFUI can also predict surgical approach [181]. In addition, urethrography provides only a two-dimensional assessment of stricture and the results may be affected by the amount of penile stretch [182], degree of pelvic rotation and patient body habitus [183]. Risks of the procedure include infection, discomfort [172], contrast reaction from intravasation of contrast [184], in addition to the risk of radiation exposure. Urethrographic clamp devices (Brodny, Knutson) are available and were found to be less painful than using the Foley catheter technique [185].
| Summary of evidence | LE |
| Retrograde urethrography is a widely available and easy to perform method of diagnosing and assessing urethral stricture but may underestimate stricture length. | 2a |
| Retrograde urethrography alone is not able to assess stricture length (or gap) in obliterative strictures or stenosis. | 2a |
| Urethrographic clamp devices are less painful than using the Foley catheter technique. | 2a |
| Recommendations | Strength rating |
| Perform retrograde urethrography to assess stricture location and length in males with urethral stricture disease being considered for reconstructive surgery. | Strong |
| Combine retrograde urethrography with voiding cystourethrography to assess (nearly) obliterative strictures, stenoses and pelvic fracture urethral injuries. | Strong |
| Use clamp devices in preference to the Foley catheter technique for urethrographic evaluation to reduce pain. | Weak |
5.2.1.e. Cystourethroscopy
Cystourethroscopy allows for accurate visual detection of a suspected stricture or can rule out a stricture as cause of obstructive voiding [186]. It can detect narrowing of the urethral lumen before changes in uroflowmetry and symptoms [151]. Cystourethroscopy can also assess the presence of LS or other pathology but cannot usually assess stricture length, as the calibre of most cystoscopes is greater than most symptomatic strictures [187]. To overcome this, the use of smaller calibre ureteroscopes (6.5Fr and 4.5Fr) has been reported [187]. This also allows an assessment of the bladder prior to surgery and may identify other pathology such as bladder stones. Cystourethroscopy is particularly helpful for diagnosing proximal BMS which may be missed on RUG [188].
Retrograde urethroscopy combined with antegrade cystoscopy via the suprapubic tract may be used to evaluate PFUI and plan the surgical approach. It allows an assessment of the length of the defect, the competence of the bladder neck, the involvement of the bladder neck in scarring, in addition to identifying the presence of bony spicules or other abnormalities (e.g. fistulae, stones) [189]. Combined retrograde and antegrade cystoscopy was found to provide similar estimates of length of urethral defect in patients with PFUI as combined retrograde and antegrade cystourethrography, but was more likely to detect fistulae, false passages, and calculi [189].
| Summary of evidence | LE |
| Cystourethroscopy will reliably detect the presence of a urethral stricture. | 3 |
| Combined retrograde urethroscopy and antegrade cystoscopy is more accurate than retrograde and voiding cystourethrography at identifying associated abnormalities such as fistulae, false passages and calculi in patients with PFUI. | 3 |
| Recommendations | Strength rating |
| Perform cystourethroscopy as an adjunct to imaging if further information is required. | Weak |
| Combine retrograde urethroscopy and antegrade cystoscopy to evaluate pelvic fracture urethral injuries as an adjunct to imaging if further information is required. | Weak |
5.2.1.f. Ultrasound
Ultrasound of the urethra or sonourethrography (SUG) provides a non-invasive three-dimensional assessment of anterior urethral stricture disease; including stricture location, length, and the degree of associated spongiofibrosis [190].
Several studies have compared SUG to RUG and cystoscopic or intraoperative findings. Sonourethrograpy was found to be more accurate at diagnosing stricture presence compared to RUG [185, 191]. Sonourethrography was also found to more accurately estimate stricture length than RUG [192]. The closest correlation for stricture length at operation was for strictures in the penile urethra [175]. Preoperative SUG findings changed the surgical plan (based on RUG) in 31% of cases, whilst intraoperative SUG findings changed the approach (based on preoperative RUG) in 19% of males undergoing anterior urethral reconstruction [183, 193]. Sonourethrography incorporating real-time elastography can provide a qualitative and quantitative assessment of spongiofibrosis [194-196]. The clinical relevance of assessing the degree of spongiofibrosis preoperatively remains to be established. Three-dimensional reconstruction of sonographic images is investigational at present [197].
The advantages of SUG are that it can be performed in the outpatient setting, provides information on the degree of spongiofibrosis and is relatively low-cost [190]. Limitations of the technique include lower sensitivity for detection of strictures in the bulbar urethra, operator dependency and the need for urethral distension requiring intraurethral anaesthesia. Sonourethrography requires specialised training in the use of US and is currently not in widespread usage.
Table 5.1: Diagnostic accuracy of sonourethrography compared to other modalities and surgical findings
| Study | N | Segment of urethra studied | Comparator | Accuracy of SUG | ||
| Diagnosis | Location | Length | ||||
| Berne-Mestre et al. 2018 [185] | 113 | Anterior and posterior | RUG, VCUG, surgical findings | SUG more accurate than RUG (p < 0.05) | - | - |
| Ravikumar et al. 2014 [191] | 40 | Anterior and posterior | RUG, VCUG, surgical findings | Anterior: SUG 100% sensitivity, 100% specificity Posterior: SUG 75% sensitivity, 50% specificity. | - | - |
| Kalabhavi et al. 2018 [176] | 30 | Anterior | RUG, surgical findings | - | - | - |
| Krukowski et al. 2018 [175] | 66 | Anterior | RUG, surgical findings | - | - | - |
N = number of patients; RUG = retrograde urethrography; SUG = sonourethrography; VCUG = voiding cystourethrogram.
5.2.1.g. Magnetic resonance imaging
Magnetic resonance imaging (MRI) has been used to image PFUIs, posterior urethral stenoses and anterior urethral strictures.
Several studies have compared MRI urethrogram to RUG and intraoperative findings. Magnetic resonance imaging urethrogram was found to be as accurate as RUG at detecting stricture site in anterior urethral strictures [198]. In terms of stricture length, both MRI urethrogram and RUG reliably correlated with intraoperative findings [198]. On the other hand, a further study of patients with anterior urethral strictures found MRI urethrogram stricture length to correlate more closely with surgical findings than RUG [199].
In a mixed group of anterior urethral strictures and posterior urethral stenoses, MRI urethrogram was as accurate (sensitivity = 100%, specificity = 91.7%) as combined RUG and sonourethrography (sensitivity = 100%, specificity = 91.7%) at diagnosing strictures [200]. There was no significant difference in the measurement of stricture length [200]. In a further study of patients with posterior urethral stenosis, MRI estimation of stenosis length correlated more closely with operative findings compared to RUG [201]. In patients with PFUI, MRI measurement of pubourethral stump angle (angle between long axis of pubis and line between the distal end of the proximal urethral stump and lower border of inferior pubic ramus) was predictive of an elaborated approach on multivariate analysis [202].
Magnetic resonance imaging was also found to be more accurate at diagnosing associated pathologies, for example, diverticula, tumours, fistulae and stones [200]. In cases of fistulation between the urinary tract and pubic symphysis after irradiation for prostate cancer, the fistula tract can be clearly demonstrated on MRI [203]. Other imaging modalities, including computed tomography (CT), may fail to identify the tract and the problem may be misdiagnosed as isolated osteomyelitis of the pubic bone leading to medical management with antibiotics rather than surgical excision [203].
The main advantage of MRI is greater anatomical detail, which is countered by the expense of the procedure and the greater complexity in interpreting images. The technique is not commonly used for routine situations, but it may be helpful in diagnosing associated pathologies which may alter patient management.
Table 5.2: Diagnostic accuracy of MRI compared to other modalities and surgical findings
| Study | N | Segment of urethra studied | Comparator | Accuracy of SUG | ||
| Diagnosis | Location | Length | ||||
| Murugesan et al. 2018 [194] | 32 | Anterior | RUG, Surgical findings | MRI and RUG equivalent (100% sensitivity, 100% specificity) | - | - |
| Fath El-Bab et al. 2015 [199] | 20 | Anterior | RUG, Surgical findings | - | - | MRI more accurate than RUG. |
| El-Ghar et al. 2010 [200] | 30 | Anterior and posterior | RUG + SUG, Surgical findings | MRI and RUG equivalent (100% sensitivity, 91.7% specificity) | - | MRI and RUG equivalent. |
| Oh et al. 2010 [201] | 25 | Posterior | RUG + SUG, Surgical findings | - | - | MRI more accurate than RUG + VCUG. |
MRI = magnetic resonance imaging; n = number of patients; RUG = retrograde urethrography; SUG = sonourethrography; VCUG = voiding cystourethrogram.
| Summary of evidence | LE |
| Magnetic resonance imaging is more accurate than retrograde urethrography and voiding cystourethrography at determining length of posterior urethral stenoses and can detect alternative associated pathologies (e.g. diverticula, fistulae). | 2a |
| Recommendation | Strength rating |
| Consider magnetic resonance imaging urethrography as an ancillary test in posterior urethral stenosis. | Strong |
Figure 5.1: Diagnostic flowchart of patients with suspected urethral stricture disease
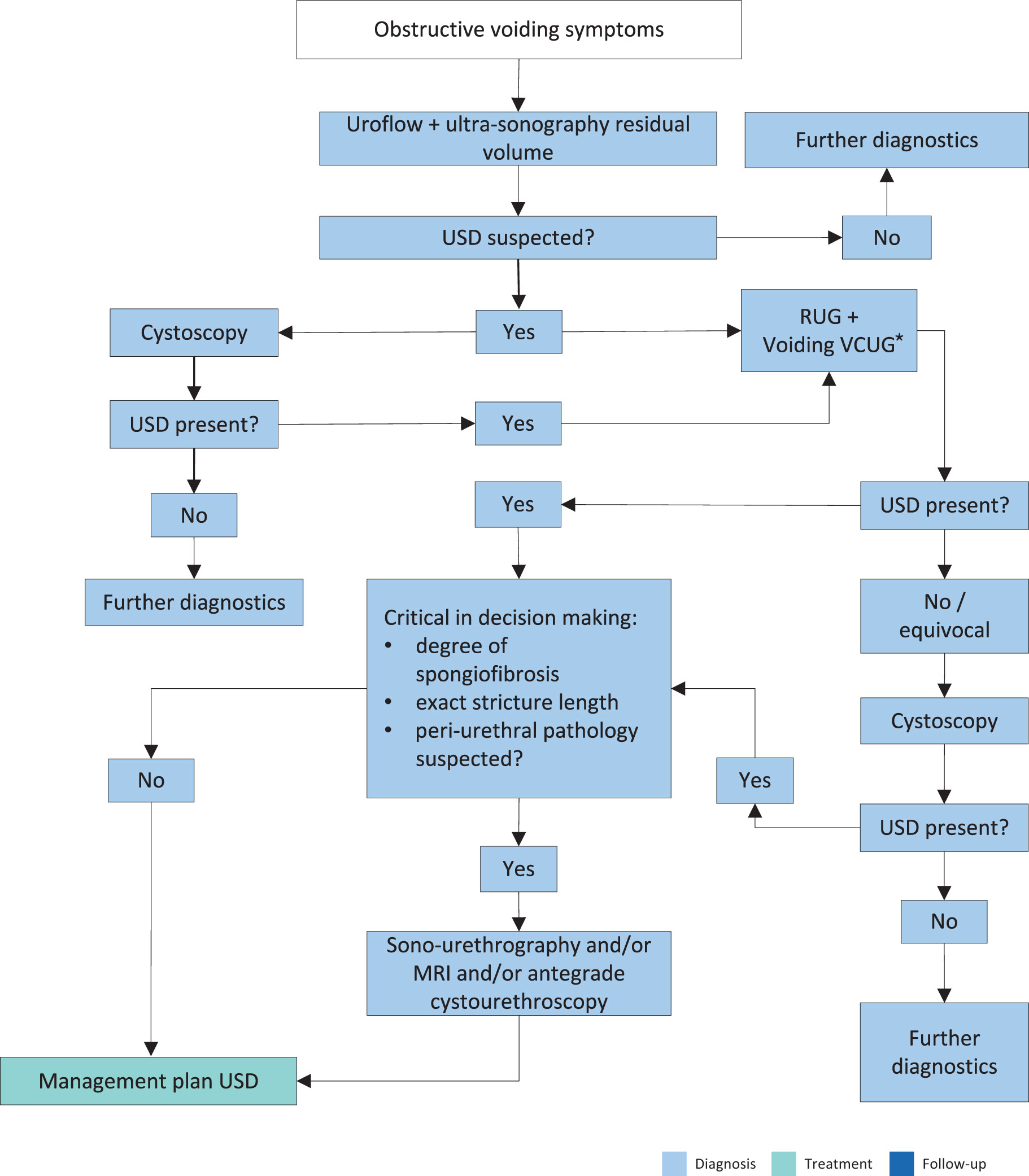 *Use VCUG in case of obliterative (or nearly obliterative) strictures or stenosis.
*Use VCUG in case of obliterative (or nearly obliterative) strictures or stenosis.
MRI = Magnetic resonance imaging; RUG = retrograde urethrography; USD = urethral stricture disease; VCUG = voiding cystourethrogram.