
How far have we come with Prostate Cancer screening in Europe? Insights from EAU26
Europe is advancing prostate cancer screening with organized, risk-adapted approaches. PRAISE-U and national pilots show that multi-step workflows using PSA, MRI, and selective biopsy are feasible, cost-effective, and well accepted by men. Clear communication, GP involvement, and digital tools are key to improving participation and early detection.
PRAISE-U: A decade of learning
The PRAISE-U initiative aims to standardize prostate cancer screening across Europe using a risk-adapted, multi-step approach informed by a decade of research. M.J. van Harten (Rotterdam, NL) opened the session by highlighting achievements so far. The project has piloted screening in multiple European regions - Galicia (ES), Ireland, Poland, Lithuania, and Manresa (ES) - and has refined algorithms for PSA testing, MRI referral, and biopsy indication.
Each pilot targeted men aged 50–69, adapting the screening process to local healthcare systems. Ireland implemented home-based PSA tests, while other regions used centralized invitations and clinical visits. Across sites, participation ranged from 13% in Ireland to 42% in Manresa, reflecting both the challenges of engaging men and the variability in national healthcare infrastructures. Despite participation challenges, pilot results suggest the PRAISE-U workflow- incorporating PSA testing, risk calculators, MRI, and selective biopsy -can effectively detect clinically significant prostate cancer while reducing unnecessary interventions.
Country-specific pilots: Key insights
Galicia, Spain: Led by R.M.F. Montero Fabuena (Ferrol, ES), Galicia piloted screening in a town of 170,000 residents, targeting 20,000 men. Invitations were sent by post with comprehensive patient information. Standard blood tests were followed by MRI for men with a 12.5% or higher calculated risk and biopsy if MRI indicated concern. Participation reached 40%, and 10% of men had elevated PSA. MRI guided biopsies in more than half of these cases, yielding an overall cancer detection rate of 71%. The study emphasized that close communication, clear workflow, and patient engagement were crucial to implementing a multi-step screening programme effectively.
Ireland: Led by D.J. Galvin (Dublin, IE), the Dublin pilot utilized home-based PSA testing kits sent by post, linked to rapid access clinics for abnormal results. Of 1,613 men recruited, 13% had abnormal PSA, 22% were deemed low-risk, and 36% avoided biopsy. While only two-thirds returned usable samples, patient feedback indicated strong acceptance of home testing, demonstrating a feasible alternative to clinic-based screening. Social campaigns, including collaboration with Movember, were essential for engagement.
Poland: In Lower Silesia, with 3.5 million inhabitants, K. Tupikowski (Wroclaw, PL) highlighted the challenges of low participation despite letters, phone calls, and text invitations. Opening additional centres and deploying a mobile “screening bus” improved engagement modestly. Lessons include the importance of local media campaigns, community-based approaches, and centralised data systems to track invitations and results effectively.
Manresa, Spain: In a population of 30,000, J. Vilaseca implemented a fully computerized invitation system through local registries, achieving a 42% participation rate. The campaign leveraged local marketing with images of doctors to encourage involvement. Technical refinements included adjusting PSA density cut-offs and refining risk calculator timing. Manresa demonstrated that integration with existing registries and community-tailored messaging can significantly enhance participation.
Lithuania: A. Patasius (Vilnius, LT) emphasized the need to avoid overdiagnosis and hyper-detection. The PRAISE-U algorithm streamlined the process with centralized call centres and defined biopsy protocols. Over a 12-month recruitment period, participation reached 23%, with 40% proceeding to biopsy and 72% diagnosed with prostate cancer. The pilot highlighted the importance of clear communication, population-specific invitations, and algorithm updates aligned with clinical guidelines.
Organised National Programmes: Sweden and Czech Republic
The Swedish OPT programme takes a pragmatic approach to organized screening, integrating it into regional public healthcare. Invitations are extended to entire birth cohorts, with PSA testing, MRI, and biopsy following a structured algorithm. O. Bratt (Gothenburg, SE) reported that organisation is more challenging than clinical decision-making; project management and communication are critical to successful implementation.
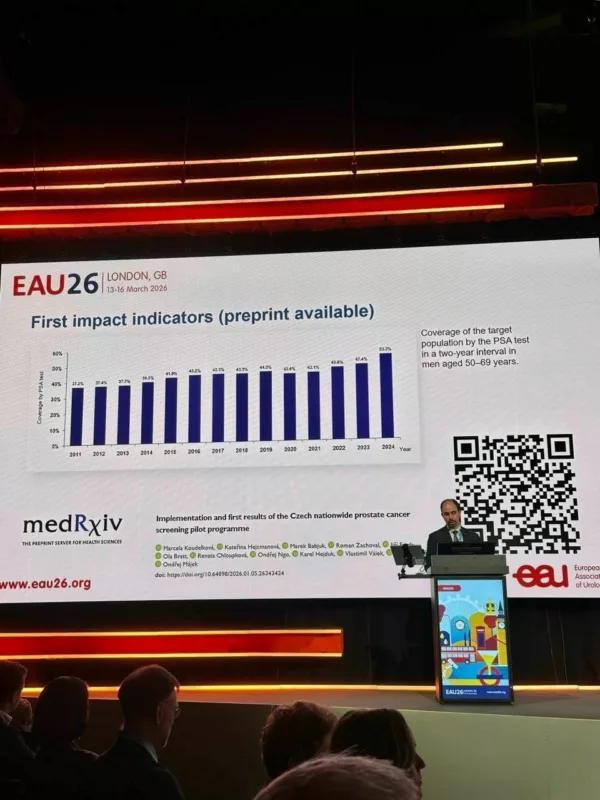
Similarly, the Czech Republic launched a nationwide pilot, enrolling approximately 240,000 men aged 50–69. Key lessons include the importance of follow-up adherence, stronger involvement of general practitioners and urologists, and leveraging digitalization for health record sharing. Performance reports for practitioners help benchmark activity and encourage compliance with screening pathways.
Cost-effectiveness and psycho-social impacts
P. Vynckier (Ghent, BE) discussed the cost-effectiveness of the PRAISE-U algorithm, using discrete-event simulation models that account for individual heterogeneity, risk stratification, and complex clinical pathways. Preliminary findings indicate that risk-adapted screening is cost-effective compared to low opportunistic testing, with lower long-term costs and improved quality-adjusted life years (QALYs).
Equally important are the psycho-social aspects. P. Kirkegaard (DK) reported that men often have moderate knowledge of prostate cancer but show positive attitudes toward screening. Stress and anxiety may increase after PSA testing but typically decline after low-risk MRI results. Family influence, trust in the healthcare system, and informed decision-making are major motivators for participation. The studies underline the need for improved patient communication and engagement strategies, particularly via general practitioners.

Comprehensive Cancer Centres and Knowledge Hubs
T. Albreht (Ljubljana, SI) discussed the evolving role of comprehensive cancer centres (CCCs) and the integration of multidisciplinary teams. These centres provide structured pathways for diagnosis and treatment, facilitating collaboration between tumour networks, regional hospitals, and European organisations such as OECI and the European Cancer Organisation.
M. Roobol (Rotterdam, NL) highlighted the PRAISE-U knowledge hub, which centralizes data from pilot studies, registries, and national programmes. By creating a large, prospective database, PRAISE-U aims to generate evidence on screening outcomes, patient pathways, and cost-effectiveness to inform EU-wide policy and recommendations.
Key challenges and future directions
Across Europe, screening pilots face common challenges: low participation rates, variability in adherence to protocols, limited engagement of general practitioners, and the technical complexity of implementing multi-step algorithms. However, lessons from PRAISE-U and national programmes suggest that structured, risk-adapted, and digitally supported approaches can improve screening effectiveness while minimizing overdiagnosis.
Future priorities include:
- Enhancing follow-up adherence and communication strategies.
- Strengthening GP involvement to ensure informed decision-making.
- Refining algorithms based on local population characteristics.
- Expanding data collection through prospective registries to support cost-effectiveness and policy decisions.
- Promoting awareness among younger men to encourage early participation.
Conclusion
The EAU26 session highlighted that Europe has made significant strides in prostate cancer screening, moving from opportunistic testing toward organized, risk-adapted approaches. PRAISE-U and national pilots provide valuable evidence for improving early detection, optimizing resource use, and minimizing patient burden. While challenges remain, the integration of clinical expertise, digital tools, patient engagement, and cross-border collaboration positions Europe to deliver more effective and equitable prostate cancer screening in the years ahead.
The session closed with a shared vision: data-driven decision-making, transparent communication, and coordinated action across healthcare systems will be essential to realize the full potential of organized prostate cancer screening in Europe.