3. EPIDEMIOLOGY AETIOLOGY AND PATHOPHYSIOLOGY
Lower urinary tract symptoms can be divided into storage, voiding and post-micturition symptoms [3], and they are prevalent, cause bother and impair QoL [4-7]. An increasing awareness of LUTS, and storage symptoms in particular, is warranted to discuss management options that could improve QoL [8]. Lower urinary tract symptoms are strongly associated with ageing [4, 5], associated costs and burden are therefore likely to increase with future demographic changes [5, 9]. Lower urinary tract symptoms are also associated with a number of modifiable risk factors, suggesting potential targets for prevention (e.g. metabolic syndrome) [10]. In addition, men with moderate-to-severe LUTS may have an increased risk of major adverse cardiac events [11].
Most elderly men have at least one LUTS [5], however, symptoms are often mild or not very bothersome [7, 8, 12]. Lower urinary tract symptoms can progress dynamically: for some individuals, LUTS persist and progress over long time periods, while for others they remit [5]. Lower urinary tract symptoms have traditionally been related to bladder outlet obstruction (BOO), most frequently when histological BPH progresses through benign prostatic enlargement (BPE) to BPO [3, 6]. However, increasing numbers of studies have shown that LUTS are often unrelated to the prostate [5, 13]. Bladder dysfunction may also cause LUTS, including DO/OAB, DU/underactive bladder (UAB), as well as other structural or functional abnormalities of the urinary tract and its surrounding tissues [13]. Prostatic inflammation also appears to play a role in BPH pathogenesis and progression [14, 15]. In addition, many nonurological conditions also contribute to urinary symptoms, especially nocturia [5].
The following list provides definitions for some of the most common conditions related to MLUTS:
- Acute retention of urine: A painful, palpable or percussible bladder when the patient is unable to pass any urine [3].
- Chronic retention of urine: A nonpainful bladder that remains palpable or percussible after the patient has passed urine. Such patients may be incontinent [3].
- Bladder outlet obstruction: The generic term for obstruction during voiding. This conditions is characterised by increasing detrusor pressure and reduced urine flow rate. Bladder outlet obstruction is usually diagnosed by invasive pressure/flow studies [3].
- Benign prostatic obstruction: A form of BOO that may be diagnosed when the cause of outflow obstruction is known to be BPE [3]. In the Guidelines, the term BPO or BOO is used as reported by the original studies.
- Benign prostatic hyperplasia: A term used (and reserved) for the typical histological pattern, which defines the disease.
- Detrusor overactivity is a urodynamic observation characterised by involuntary detrusor contractions during the filling phase, which may be spontaneous or provoked [3]. DO is usually associated with OAB syndrome characterised by urinary urgency, with or without urge urinary incontinence (UUI), usually with increased daytime frequency and nocturia, if there is no proven infection or other obvious pathology [16].
- Detrusor underactivity during voiding is characterised by decreased detrusor voiding pressure leading to a reduced urine flow rate. Detrusor underactivity causes UAB syndrome which is characterised by voiding symptoms similar to those caused by BPO [17].
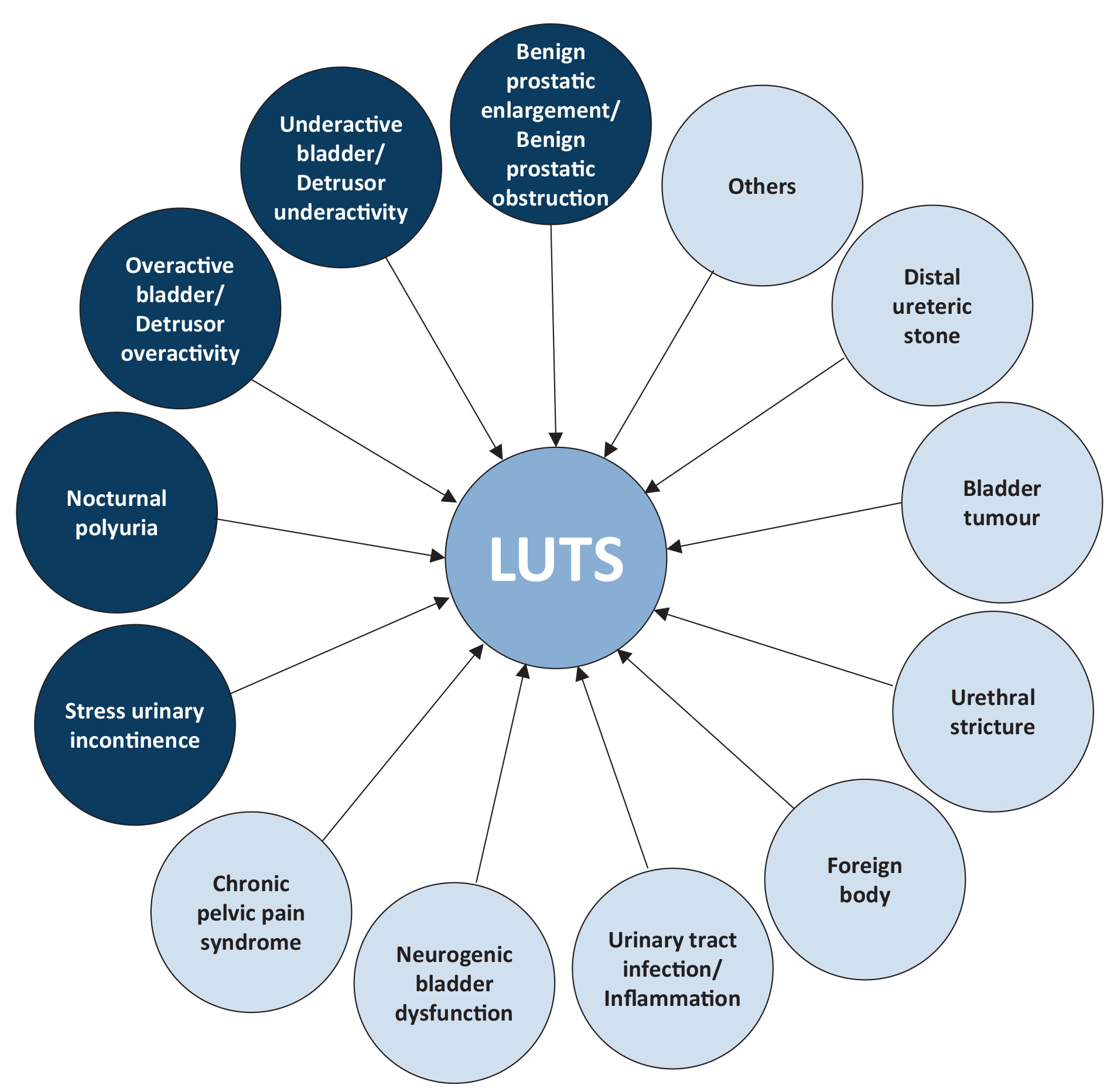
Figure 1 illustrates the potential causes of LUTS. In any man complaining of LUTS, it is common for more than one of these factors to be present.
Figure 1: Causes of MLUTS