
8. PENILE CURVATURE
8.1. Congenital penile curvature
8.1.1. Epidemiology, aetiology and pathophysiology
Congenital penile curvature (CPC) is a rare condition with a reported incidence of < 1% [915], although some studies have reported higher prevalence rates of 4-10% in the absence of hypospadias [916]. Congenital penile curvature results from disproportionate development of the tunica albuginea of the corporal bodies and is not associated with urethral malformation. In most cases, the curvature is ventral, but it can also be lateral or, more rarely, dorsal [917].
8.1.2. Diagnostic evaluation
Taking a medical and sexual history is usually sufficient to establish a diagnosis of CPC. Patients usually present after reaching puberty, as the curvature becomes more apparent with erections and sexual activity. More severe curvatures can make intercourse difficult or impossible. Physical examination and photographic documentation during erection (preferably after intracavernous injection of vasoactive drugs) are both mandatory to document the curvature and exclude other pathologies [917].
8.1.3. Disease management
Surgery is the definitive treatment for this disorder and can be deferred until after puberty. A survey suggested that men with untreated ventral penile curvature report greater dissatisfaction with penile appearance, increased difficulty during intercourse, and psychological problems. These findings have been used to support surgical correction of CPC in childhood, although early surgery should be discouraged as penile growth is not yet complete [918]. Surgical treatments for CPC generally share the same principles as in PD. Plication techniques (Nesbit, 16-dot, Yachia, Essed-Schröeder and others) with or without neurovascular bundle elevation (medial/lateral) and complete penile degloving, have been described [919-928]. Other approaches are based on corporal body derotation with various technical refinements that enable correction of a ventral curvature, with reported minimal narrowing and shortening [929-932]. There are no direct comparative studies; therefore, no single technique can be recommended for surgical correction.
8.1.4. Summary of evidence and recommendation for diagnosis and treatment of congenital penile curvature
| Summary of evidence | LE |
| Medical and sexual history are usually sufficient to establish a diagnosis of CPC. Physical examination and photographic documentation during erection (preferably after intracavernous injection of vasoactive drugs) are mandatory to document the curvature. | 3 |
| Surgery is the only treatment option for CPC, which should be deferred until after puberty and performed at any time in adult life in individuals with significant functional impairment during intercourse. | 3 |
| Recommendation | Strength rating |
| Use the Nesbit/Yachia procedure or plication techniques with or without neurovascular bundle dissection (medial/lateral) for satisfactory curvature correction. | Strong |
8.2. Peyronie’s Disease
A discussion on the aetiology, risk factors and pathophysiology of PD can be found in Appendix 4 of the online supplementary evidence.
8.2.1. Epidemiology
Epidemiological data on PD are limited. Prevalence rates of 0.1-20.3% have been reported, with a higher prevalence in patients with ED and diabetes [933-944]. Incidence rate of PD in population >18 years old is 19.6-23 cases per 100,000 per year [944]. A survey has indicated that the prevalence of definitive and probable cases of PD in the USA is 0.7% and 11%, respectively, suggesting that PD is an underdiagnosed condition [945]. Peyronie’s disease often occurs in older males with a typical age of onset of 50-60 years. However, PD also occurs in younger males (< 40 years), with a reported prevalence of 1.5-16.9% [937,946,947].
8.2.2. Diagnostic evaluation
The aim of the initial evaluation is to obtain information on the presenting symptoms and their duration (e.g. pain on erection, palpable nodules, deformity, length and girth, and EF). It is important to obtain information on the distress caused by the symptoms and the potential risk factors for ED and PD. A disease-specific questionnaire (PD questionnaire [PDQ]) has been developed for use in clinical practice and trials. The PDQ measures three domains, including psychological and physical symptoms, penile pain and symptom bother [948].
Clinicians should take a focused history to distinguish between active and stable disease, as this will influence medical treatment and timing of surgery. Patients who are still likely to have active disease are those with a shorter symptom duration, pain on erection, or a recent change in penile deformity. Resolution of pain and stability of the curvature for at least three months are accepted criteria of disease stabilisation as well as patients’ referral for specific medical therapy [949,950] or surgical intervention, if indicated [951].
The examination should start with a focused genital assessment that is extended to the hands and feet for detecting possible Dupuytren’s contracture or Ledderhosen scarring of the plantar fascia [952]. Penile examination is performed to assess the presence of a palpable nodule or plaque. There is no correlation between plaque size and degree of curvature [953]. Measurement of the stretched or erect penile length is important, because it may have an impact on the subsequent treatment decisions and potential medico-legal implications [954-956].
An objective assessment of penile curvature with an erection is mandatory. This can be obtained by several approaches, including home self-photography of a natural erection (preferably), using a vacuum-assisted erection test or an intracavernous injection using vasoactive agents. However, it has been suggested that the intracavernous injection method is superior, as it is able to induce an erection similar to or better than that which the patient would experience when sexually aroused [957-959]. Computed tomography and MRI have a limited role in the diagnosis of the curvature and are not recommended on a routine basis. Erectile function can be assessed using validated instruments such as the IIEF, although this has not been validated in PD patients [960]. Erectile dysfunction is common in patients with PD (30-70.6%) [961,962]. The presence of ED and psychological factors may also have a profound impact on the chosen treatment strategy [963]. Ultrasound measurement of plaque size is not accurate but may be helpful to assess the presence of the plaque, its calcification and location [964,965]. Doppler US may be used to assess penile haemodynamic and ED aetiology [962], particularly penile arterial inflow, in the context of planned interventional modality (e.g. plaque incision and grafting) to exclude arteriogenic ED.
8.2.2.a. Summary of evidence and recommendations for diagnosis of Peyronie’s disease
| Summary of evidence | LE |
| Ultrasound measurement of plaque size is inaccurate and operator-dependent. | 3 |
| Doppler US may be used to assess penile haemodynamic and vascular anatomy. | 2a |
| Intracavernous injection method is superior to other methods to provide an objective assessment of penile curvature with an erection. | 4 |
| Recommendations | Strength rating |
| Take a medical and sexual history of patients with Peyronie’s disease (PD), include duration of the disease, pain on erection, penile deformity, difficulty in vaginal/anal intromission due to the deformity and erectile dysfunction (ED). | Strong |
| Perform a physical examination, including assessment of palpable plaques, stretched or erect penile length, degree of curvature (self-photography, vacuum-assisted erection test or pharmacological-induced erection) and any other related diseases (e.g. Dupuytren’s contracture, Ledderhose disease) in patients with PD. | Strong |
| Use the PD specific questionnaire, especially in clinical trials, but routine use in daily clinical practice is not mandatory. | Weak |
| Use penile Doppler US in the case of diagnostic evaluation of ED to evaluate penile haemodynamic especially prior to surgery. | Weak |
8.2.3. Disease management
8.2.3.a. Conservative treatment
Conservative treatment of PD is primarily focused on patients in the early stage of the disease as an adjunct treatment to relieve pain and prevent disease progression, or if the patient declines other treatment options during the active phase [951,952]. Several options have been suggested, including oral pharmacotherapy, intralesional injection therapy, shockwave therapy and others. The results of the studies on conservative treatment for PD are often contradictory, making it difficult to provide recommendations in everyday, real-life settings [966,967].
8.2.3.a.1. Oral treatment
Phosphodiesterase type 5 inhibitors
Phosphodiesterase type 5 inhibitors were first suggested as a treatment for PD in 2003 to reduce collagen deposition and increase apoptosis through the inhibition of transforming growth factor (TGF)-b1 [968-970]. Retrospective studies shown that sildenafil 25mg and tadalafil 5mg daily were able to reduce pain during the active phase of the disease with some improvements, including in terms of curvature decrease [971-973]. Findings from an observational retrospective study including patients in the acute phase of PD and ED who had been treated with Tadalafil 5mg once daily compared to patients with comparable baseline parameters who decided not to take the daily compound (i.e. 108 intervention vs. 83 controls) showed that treated men had lower curvature progression rates at 12 weeks (25.9% vs. 39.7%; p = 0.042) [974]. Similarly, mean SHIM score and PDQ-Overall and PDQ-Penile Pain scores significantly improved in the intervention group (p < 0.001).
Nonsteroidal anti-inflammatory drugs
In patients with active-phase PD, nonsteroidal anti-inflammatory drugs (NSAIDs) may be considered for the management of penile pain. Regular reassessment of pain severity and careful monitoring of therapeutic effectiveness are recommended throughout treatment.
8.2.3.a.2. Intralesional treatment
Injection of pharmacologically active agents directly into penile plaques represents another treatment option. It allows a localised delivery of a pharmacological agent that provides higher concentrations of the drug inside the plaque. Several drugs have been investigated over the last two decades. Among them, steroids and botulinum toxin are not discussed in this chapter, given the poor quality of the available evidence showing no significant effect in patients with PD.
Calcium channel antagonists: verapamil and nicardipine
The rationale for intralesional use of channel antagonists in patients with PD is based on in vitro research [975,976]. Due to the use of different dosing schedules and the contradictory results obtained in published studies, the evidence is not strong enough to support the clinical use of injected channel blockers verapamil and nicardipine, and the results do not demonstrate a meaningful improvement in penile curvature compared to placebo [977-982]. In fact, most of the studies did not perform direct statistical comparison between these groups.
Collagenase of Clostridium histolyticum
Collagenase of Clostridium histolyticum (CCH) is a chromatographically purified bacterial enzyme that selectively targets collagen, the primary component of the PD plaque [983-986]. In 2014, the EMA-approved CCH for the non-surgical treatment of the stable phase of PD in men with palpable dorsal plaques in whom abnormal curvature of 30-90o and non-ventrally located plaques are present [987,988]. However, CCH has been officially withdrawn from the European market by its manufacturer. Despite this, the evidence and recommendations for CCH have been maintained in these Guidelines for completeness.
The original treatment protocol in all studies consists of two injections of 0.58mg of CCH 24-72 hours apart every six weeks for up to four cycles. Data from IMPRESS (Investigation for Maximal Peyronie´s Reduction Efficacy and Safety Studies) I and II studies [989], as well as post-approval trials [990], demonstrated the efficacy and safety of this treatment, and are summarised in Table S8.2 and in Appendix 4 of the online supplementary evidence.
The average improvement in curvature was 34% compared to 18.2% in the placebo group. Three adverse events of corporeal rupture were surgically repaired. The greatest chance of curvature improvement was for curvatures between 30° and 60°, longer duration of disease, IIEF > 17, and no calcification [950]. An 18.2% improvement from baseline in the placebo arm was also observed. These findings raise questions regarding the proposed role of plaque injection and penile modelling, regardless of the medication, in improving outcomes in men with PD, as the placebo or modelling arm resulted in relatively high curvature reduction compared to the treatment arm.
The conclusion of the IMPRESS I and II studies is that that CCH improves PD both physically and psychologically [991]. A post hoc meta-analysis of the IMPRESS studies demonstrated better results in patients with curvatures < 60o, > two years of onset, no calcification in the plaque and good EF [990].
A modified short protocol consisting of administration of a single (0.9mg, one vial) injection per cycle distributed along three lines around the point of maximum curvature up to three cycles, separated by four-weekly intervals, has been proposed and rapidly popularised replacing physician modelling with a multi-modal approach through penile stretching, modelling and VED at home [992]. The results from this modified protocol were comparable to the results of the IMPRESS trials and appeared to decrease the cost and duration of treatment [993]. A nomogram developed to predict treatment success after CCH for PD showed that patients with longer PD duration, greater baseline penile curvature and basal plaque location had a greater chance of treatment success [994]; however, these findings need to be externally validated. Data from a prospectively maintained registry including 228 patients showed that even men with ventral curvature showed up to 49% curvature improvement [995].
Regarding safety concerns, most PD patients treated with CCH experienced at least one mild or moderate TRAE localised to the penis (penile haematoma [50.2%], penile pain [33.5%], penile swelling [28.9%], and injection site pain [24.1%]), which resolved spontaneously within 14 days of injection [996]. The adverse reaction profile was similar after each injection, regardless of the number of injections administered. Other authors proposed that a specific technique of CCH injection (the 'fan' technique) may reduce the risk of penile hematoma [997]. Serious TEAEs (0.9%) included penile haematoma and corporeal rupture that require surgical treatment. According to IMPRESS data and the shortened protocol, to prevent serious TEAEs, men should be advised to avoid sexual intercourse in the four weeks following injection. Preliminary data suggest that treatment in the acute phase of the disease is effective and safe [960,998-1003].
In conclusion, CCH is a safe and established treatment for stable-phase disease with evidence suggesting that CCH also has a role in affecting the progression of active-phase disease. There is a large effect of traction or modelling in controlled studies, whilst studies reporting on modified protocols have small numbers of patients and are largely uncontrolled. Patients should be counselled fully on the efficacy of collagenase and the high cost of treatment.
It has been suggested that patients with severe curvature may benefit from CCH injections because of a potential downgrading of the penile curvature: a decrease in curvature may allow for a penile plication procedure instead of a plaque incision and grafting procedure, avoiding the more negative impact on EF. In an RCT comparing patients submitted to CCH and penile traction therapy (PTT) versus surgery and PTT, men with > 30° curvature who underwent treatment with CCH experienced lesser curvature improvements but greater overall orgasmic function, penile length, subjective EF, and penile sensation compared to surgery [1004]. Further studies are required to validate these initial findings [960,1002]. In a large retrospective series, surgery after CCH injections appeared more likely in patients with complex curvature, above 60°, without increased risk of complications [1005].
Interferon α-2b
In two published RCTs analysing data from the same cohort, intralesional injections of IFN-α2b significantly improved penile curvature, plaque size and density, and pain, compared to placebo [988,1006,1007]. Overall, 50 patients were treated with IFN-α2b injections as compared to 63 patients receiving placebo injections. The mean curvature improvement in the treatment group was 13.5°. Patients reported mild adverse effects, which include sinusitis and flu-like symptoms, which can be effectively treated with NSAIDs. Given the limited evidence, and the withdrawal of IFN-α2b from the European and USA markets in 2021, this treatment is not recommended for patients with PD.
Hyaluronic acid
The effect of HA treatment in patients with acute phase PD has been investigated in a small case-control non-randomised study, in one single arm trial, in one comparative non-randomised study and in two non-placebo-controlled RCTs. In these studies, significant improvement of pain, curvature and IIEF-15 was observed as compared with no treatment and verapamil [977,1008-1010]. In an RCT, oral administration of HA combined with intralesional injection was found to be superior to intralesional injection only and an improvement of 7.8 ± 3.9 degrees in curvature and reduction in plaque size of 3.0mm was observed [1011]. In a single-arm study, HA injections also appear to have a positive effect in patients with chronic PD [1012]. A summary of available studies can be found in Table S8.3 in Appendix 4 of the online supplementary evidence. The lack of data from placebo-controlled RCT does not allow a conclusion on the efficacy of this treatment.
Platelet rich plasma (PRP)
Few single-arm, non-comparative studies in patients with both stable and acute PD have evaluated the effect of PRP on penile curvature, plaque size, PDQ and IIEF [989,1013-1019] Overall, data show a positive effect on curvature with a mean improvement ranging from 10 to 16° [1019]. However, the effect of PRP in patients with PD remains to be proven, given the lack of placebo-controlled data. An ongoing phase IIb, randomised, placebo-controlled crossover trial enrolled 25 patients with a planned target of 80 men with PD: the first ongoing data on nine patients in treatment group versus 14 in placebo group showed a significant improvement of penile curvature at six months in the group receiving the sequence PRP-placebo as compared to those receiving placebo-PRP [1020]. This may suggest a delayed effect of PRP on curvature improvement, but data remains preliminary. A summary of available studies can be found in Table S8.3 in Appendix 4 of the online supplementary evidence.
8.2.3.a.3. Other treatments
Extracorporeal shockwave treatment
The mechanism of action involved in extracorporeal shockwave treatment (ESWT) for PD is still unclear. Five RCTs and two meta-analyses [1021-1027] assessed the efficacy of ESWT for PD. Three were sham-controlled trials, while one compared ESWT with the combination of ESWT and PDE5I (tadalafil) [1028].
All trials showed positive findings in terms of pain relief, but no effect on penile curvature and plaque size. Inclusion criteria varied widely among studies and further investigation is needed. Therefore, ESWT should not be used as a primary treatment for penile curvature in men with PD. The results are summarised in Table S8.4 in Appendix 4 of the online supplementary evidence.
Penile traction therapy
In men with PD, potential mechanisms for disease modification with PTT have been proposed, including collagen remodelling via decreased myofibroblast activity and matrix metalloproteinase up-regulation [1029,1030].
The stated clinical goals of PTT are to non-surgically reduce curvature, enhance girth, and recover lost length, which are attractive to patients with PD. However, clinical evidence is limited due to the small number of patients included, the heterogeneity in the study designs, and the non-standardised inclusion and exclusion criteria, which make it impossible to draw any definitive conclusions about PTT [1031-1035].
In a meta-analysis including five randomised and non-randomised controlled trials, the use of PTT was associated with a significant improvement in penile curvature of about 15° [1036]. The effect of PTT in patients with calcified plaques, hourglass or hinge deformities, which are, theoretically, less likely to respond to PTT, has not been systematically studied. The treatment can result in discomfort and be inconvenient, as the device needs to be used for an extended period (two to eight hours daily), but has been shown to be tolerated by highly motivated patients. There were no reported serious adverse effects, including skin changes, ulcerations, hypo-aesthesia or diminished rigidity [1033,1037]. A summary of the clinical evidence for PTT can be found in Table S8.5 in Appendix 4 of the online supplementary evidence.
In conclusion, PTT seems to be effective and safe for patients with PD [1038], but there is a lack of evidence to provide a definitive recommendation for its use as a monotherapy for PD.
Vacuum erection device
Vacuum erection device therapy results in dilation of cavernous sinuses, decreased retrograde venous blood flow and increased arterial inflow [1039]. Intracorporeal molecular markers are affected by VED application, including decreases in hypoxia-inducible factor-1α, TGF-β1, collagenase, and apoptosis, and increases endothelial nitric oxide synthase (eNOS) and α-smooth muscle actin, given their role in the pathogenesis of PD [1040]. Only two retrospective studies assessed the efficacy of VED therapy in mechanically straightening the penile curvature of PD as monotherapy and further studies are needed [1041,1042].
Multimodal treatment
There is some evidence suggesting that a combination of different oral agents can be used for treatment of the acute phase of PD. However, there does not seem to be a consensus on which drugs to combine or the optimum drug dosage, nor has there been a comparison of different drug combinations.
A long-term study assessing the role of multimodal medical therapy (injectable verapamil associated with antioxidants and local diclofenac) demonstrated that treatment was efficacious for PD patients. The study concluded that combination therapy reduced pain more effectively than verapamil alone, making this specific combination treatment more effective compared to monotherapy [1040]. Furthermore, combination protocols including injectable therapies, such as CCH, have been studied in controlled trials. The addition of adjunctive PTT and VED has been described; however, limited data are available regarding their use [1043].
Penile traction therapy has been evaluated as an adjunct therapy to intralesional injections with interferon, verapamil or CCH [978,1044-1047]. These studies showed conflicting results in terms of improvement in penile length or curvature. However, data showed a 0.4cm to 1.8cm length increase among men using the devices for > 3 hours/day and a greater improvement of curvature [1045]. A meta-analysis demonstrated that men who used PTT as an adjunct to surgery or injection therapy for PD had, on average, an increase in stretched penile length (SPL) of 1cm compared to men who did not use adjunctive PTT. There was no significant change in curvature between the two groups [1048].
In another meta-analysis, the combined treatment of CCH and the use of VED or PTT between injection intervals resulted in an additional decrease of 0.3 in penile curvature and in an increase of 0.5cm in penile length compared with CCH monotherapy [1049]. Data have suggested that combination of PDE5I (sildenafil 25mg twice daily) after CCH treatment (shortened protocol combined with VED) is superior to CCH alone for improving penile curvature and EF [1050]. Further studies are necessary to externally validate those findings.
8.2.3.a.4. Summary of evidence and recommendations for conservative treatment of Peyronie’s disease
| Summary of evidence | LE |
| Conservative treatment for PD is primarily aimed at treating patients in the early stage of the disease to relieve symptoms and prevent progression. | 3c |
| Nonsteroidal anti-inflammatory drugs can be used to treat pain in the acute phase. | 4 |
| Contradictory evidence is available for intralesional treatment with calcium channel antagonists: verapamil and nicardipine. | 3c |
| Intralesional treatment with collagenase clostridium histolyticum showed significant decreases in penile curvature, plaque diameter and plaque length in men with acute and stable disease. | 1b |
| Intralesional treatment with interferon may improve penile curvature, plaque size, density and pain. | 2b |
| Intralesional HA improves pain, stop disease progression and may improve curvature in patients with acute phase PD. | 3b |
| Extracorporeal shockwave treatment may be offered to treat penile pain, but it does not improve penile curvature and plaque size. | 2b |
| Treatment with PTT alone or in combination with injectable therapy as part of a multimodal approach may reduce penile curvature and increase penile length, although the available studies have considerable limitations. | 2b |
| Recommendation | Strength rating |
| Fully counsel patients regarding all available treatment options and outcomes before starting any treatment. | Strong |
| Offer conservative treatment to patients not fit for surgery or when surgery is not acceptable to the patient. | Strong |
| Use nonsteroidal anti-inflammatory drugs to treat penile pain in the acute phase of PD. | Strong |
| Use extracorporeal shockwave treatment (ESWT) to treat penile pain in the acute phase of Peyronie’s disease (PD). | Weak |
| Use phosphodiesterase type 5 inhibitors to treat concomitant erectile dysfunction. | Weak |
| Use intralesional hyaluronic acid either alone or in combination with other treatments to reduce pain and/or penile curvature in acute phase PD, although outcome data are still limited. | Weak |
| Use intralesional therapy with collagenase clostridium histolyticum in patients with PD and dorsal or lateral curvature > 30˚, who request non-surgical treatment. | Strong |
| Fully counsel patients that data on the use of intralesional platelet-rich plasma, either alone or in combination with oral treatment, to reduce pain or penile curvature, are still limited. | Strong |
| Do not use ESWT to improve penile curvature. | Strong |
| Offer penile traction devices and vacuum devices to reduce penile deformity or as part of a multimodal therapy approach, although outcome data is limited. | Weak |
8.2.3.b. Surgical treatment
Although conservative treatment for PD may resolve painful erections in most men, only a small percentage experience significant straightening of the penis. The aim of surgery is to correct curvature and allow penetrative intercourse. Surgery is indicated in patients with significant penile deformity and difficulty with intercourse associated with sexual bother. Patients must have a stable disease for three to six months (or more than 9-12 months after onset of PD) [951,1051,1052]. In addition, there are other situations that may precipitate an indication for surgery when the disease is stable, such as failed conservative or medical therapies, extensive penile plaques or patient preference [1053,1054].
Before considering reconstructive surgery, it is recommended to document the size and location of penile plaques, penile length, the presence or absence of ED, the degree of curvature, and complex deformities. Approximately 10% of PD patients will have atypical features, including ventral plaque, ossified plaque, hourglass deformity, unilateral indentations, severely shortened penile length and multiplanar curvatures
[1055,1056].
The potential aims and risks of surgery should be fully discussed with the patient so that they can make an informed decision [1052]. Specific issues to mention during this discussion are: risk of penile shortening, ED, penile numbness and delayed orgasm, the risk of recurrent curvature, potential for palpation of knots and stitches underneath the skin, potential need for circumcision at the time of surgery, residual curvature, and the risk of further penile wasting with shortening procedures [951,1057]. Selection of the most appropriate surgical intervention is based on penile length assessment, curvature severity and EF status, including response to pharmacotherapy in cases of ED [951]. Patient expectations from surgery must also be included in the preoperative assessment. The main objective of surgery is to achieve a 'functionally straight' penis, and this must be fully understood by the patient to achieve the best possible satisfaction outcomes after surgery
[1052,1058].
Three major types of reconstruction may be considered for PD: (i) tunical shortening procedures; (ii) tunical lengthening procedures; and (iii) PPI, with or without straightening techniques in the presence of concomitant ED and residual curvature [1059,1060].
Penile degloving with associated circumcision (as a means of preventing postoperative phimosis) should be considered the standard approach for all types of procedures, although modifications have been described. Only one study has suggested that circumcision is not always necessary (e.g. in cases where the foreskin is normal preoperatively) [1061]. Non-degloving techniques have been described that prevent ischaemia and lymphatic complications after subcoronal circumcision [1062,1063].
There are no standardised questionnaires for the evaluation of surgical outcomes. Data from well-designed prospective studies are scarce, with low levels of evidence. Data are mainly based on retrospective single-centre studies, typically non-comparative and non-randomised, or on expert opinion [951,1064]. Therefore, surgical outcomes must be treated with caution.
8.2.3.b.1. Tunical shortening procedures
Tunical shortening procedures achieve straightening of the penis by shortening the longer, convex side of the penis. For men with good EF, adequate penile length, without complex deformities, such as an hourglass or hinge type narrowing abnormalities, and non-severe curvature, a tunical shortening procedure can be considered an appropriate surgical approach. Numerous techniques have been described, although they can be classified as excisional, incisional and plication techniques. The Nesbit procedure operation is based on an elliptical excision of tunica albuginea opposite to the point of maximum curvature [1065,1066].
The Yachia technique is based on a completely different concept, as it utilises the Heinke-Mikowitz principle for which a longitudinal tunical incision is closed transversely to shorten the convex side of the penis. This technique, initially described by Lemberger in 1984, was popularised by Yachia in 1990, when he reported a series of ten cases [1067-1072].
Pure plication techniques are simpler to perform. They are based on single or multiple plications performed without making excisions or incisions on the tunical albuginea to limit the potential damage to the veno-occlusive mechanism [954,1073-1089]. Another modification described the ‘16-dot’ technique that consists of the application of two pairs of parallel Essed-Schroeder plications, tensioned more or less depending on the degree of curvature [1090-1093]. Results and satisfaction rates are similar for both incision/excision techniques.
In general, using these tunical-shortening techniques, complete penile straightening is achieved in > 85% of patients. Recurrence of the curvature and penile hypo-aesthesia is uncommon (~10%) and the risk of postoperative ED is low. Penile shortening is the most commonly reported adverse outcome of these procedures. Shortening of 1-1.5cm has been reported for 22-69% of patients, which is rarely the cause of postoperative sexual dysfunction and patients may perceive the loss of length as greater than it is. It is therefore strongly advisable to measure and document the penile length perioperatively, both before and after the straightening procedure, whichever the technique used (Table 8.2).
In studies, it has been shown that, in patients with hourglass deformity or hinge deformity with/without penile curvature, the indentation can be corrected with extra-tunical grafting. Since the tunica albuginea is not compromised in this technique, the risk of ED is lower compared to grafting procedures (0-2.9%) and satisfaction rate is up to 85.7-100% [1094-1097].
As previously noted, multiple techniques with small procedural modifications have been described, all of which are supported exclusively by retrospective studies. The absence of adequately designed comparative analyses among these techniques results in an overall low level of evidence, precluding the recommendation of any single method over the others.
Table 8.2: Results of tunical shortening procedures for Peyronie’s Disease (data from various, non-comparable studies) [954, 1067-1090, 1098-1104]
| Tunical shortening procedures | |||||
| Nesbit | Modified Nesbit | Yachia | 16-dot / mod16-dot | Simple plication | |
| No. of patients/studies | 652 / 4 | 387 / 5 413/6 | 150 / 6 | 285 / 5 | 1068 / 18 1173 / 20 |
| Significant penile shortening (%)*† | 8.7% (5-39) | 3.2% 4.8% (0-13) | 3.5% (0-10) | 5.9% (0-6) | 8.9% (0-55) 9.2% (0-55) |
| Any penile shortening (%)* | 21.8% (9-39) | 58.% 56.9% (23-74) | 69% (47-97) | 44.6% (40-52) | 33.4% (0-90) |
| Penile straightening (%)* | 88.5% (86-100) | 97.6% 97.1% (92-100) | 95.5% (93-100) | 96.9% (95-100) | 94.2% (85-100) |
| Postoperative de novo ED (%)* | 6.9% (0-17) | 3% 5% (0-13) | 9.6% (0-13) | 3.8% (0-13) | 8.8% (0-38) |
| Penile hypoesthesia (%)* | 11. 8% (2-60) | 5.6% 7.7% (0-31) | 1% (0-3) | 8.2% (6-13) | 9% (0-47) |
| Overall satisfaction (%)* | 83.5% (76-88) | 93.4% (87-100) | 86.8% (78-100) | 94% (86-100) | 85.2% (52-100) |
| Follow-up (months)* | (69-84) | (19-42) (19-102) | (10-24) | (18-71) | (12-141) |
*Data are expressed as weighted average. † Defined as > 30 degrees of curvature. Ranges are in parentheses. ED = erectile dysfunction.
8.2.3.b.2. Tunical lengthening procedures
Tunical lengthening procedures are performed on the concave side of the penis at the point of maximum curvature that usually coincides with the location of the plaque, an incision is made, creating a defect in the albuginea that is covered with a graft. Although tunical lengthening procedures rarely lead to long-term penile length gain, they aim to minimise penile shortening caused by plication of the tunica albuginea and correct complex deformities. In practice, tunical lengthening procedures are often combined with penile plication or shortening procedures to correct residual curvature and therefore may also result in penile shortening [1105]. Tunical lengthening surgery is preferable in patients with significant penile shortening, severe curvature and/or complex deformities (hourglass or hinge) but without underlying ED. The definition of severe curvature has been proposed to be > 60o, although no studies have validated this threshold. On the concave side of the penis, at the point of maximum curvature, which usually coincides with the location of the plaque, an incision is made, creating a defect in the albuginea that is covered with a graft. Complete plaque removal or plaque excision may be associated with higher rates of postoperative ED due to venous leak, but partial excision in cases of florid calcification may be permissible [1106,1107]. Patients who do not have preoperative ED should be informed of the significant risk of postoperative ED of up to 50% [1057].
Many different grafts have been used. The ideal graft should be resistant to traction, easy to suture and manipulate, flexible (although not too much, to avoid aneurysmal dilations), readily available, cost-effective, and morbidity should be minimal, especially when using autografts. No graft material meets all these requirements. Moreover, the studies performed did not compare different types of grafts and biomaterials and were often single-centre retrospective studies, so there is not a single graft that can be recommended for surgeons [1108]. The use of geometric principles introduced by Egydio may help to determine the exact site of the incision, and the shape and size of the defect to be grafted [1109].
Grafts for PD surgery can be classified into four types [1110]:
- Autografts: taken from the individual themselves, they include the dermis, vein, temporalis fascia, fascia lata, tunica vaginalis, tunica albuginea and buccal mucosa.
- Allografts: also of human origin but from a deceased donor, including the pericardium, fascia lata and dura mater.
- Xenografts: extracted from various animal species and tissues, including bovine pericardium, porcine small intestinal submucosa, bovine and porcine dermis, and TachoSil® (matrix of equine collagen).
- Synthetic grafts: these include Dacron® and Gore-Tex®.
All the autologous grafts have the inconvenience of possible graft harvesting complications. Dermal grafts are commonly associated with veno-occlusive ED (20%) due to lack of adaptability, so they have not been used in contemporary series [1108,1111-1122]. Vein grafts have the theoretical advantage of endothelial-to-endothelial contact when grafted to underlying cavernosal tissue. The saphenous vein has been the most used vein graft [1123-1138]. For some extensive albuginea defects, more than one incision may be needed. Tunica albuginea grafts have perfect histological properties but some limitations: the size that can be harvested, the risk of weakening penile support, and making future procedures (PPI) more complicated [1139-1141].
Grafting with tunica vaginalis has reportedly yielded improved outcomes when vascularised tissue is utilised; nonetheless, graft harvesting may adversely affect paratesticular structures [1142-1146]. On the premise that placement of the submucosal surface in direct contact with the corpus cavernosum enhances graft vascularisation and integration, buccal mucosal grafts - despite their stratified squamous epithelial composition – have gained attention, with favourable short-term outcomes reported [1147-1153].
Cadaveric dura mater is no longer used due to concerns about the possibility of infection [1154,1155]. Cadaveric pericardium (Tutoplast©) offers good results by coupling excellent tensile strength and multidirectional elasticity/expansion by 30% [1032,1107,1118,1156,1157]. Cadaveric or autologous fascia lata or temporalis fascia offers biological stability and mechanical resistance [1158-1160].
Xenografts have become more popular. Small intestinal submucosa, a type I collagen-based xenogenic graft derived from the submucosal layer of the porcine small intestine, has been shown to promote tissue-specific regeneration and angiogenesis, and support host cell migration, differentiation and growth of endothelial cells, resulting in tissue that is structurally and functionally similar to the original [1161-1170]. As mentioned above, pericardium (bovine, in this case) has good traction resistance and adaptability, and good host tolerance [1138,1171-1174]. Grafting by collagen fleece (TachoSil©) in PD has some major advantages such as decreased operating times, easy application and an additional haemostatic effect, but the residual deformity cannot be assessed perioperatively [1175-1180].
It is generally recommended that synthetic grafts, including polyester (Dacron®) and polytetrafluoroethylene (Gore-Tex®), are avoided due to increased risks of infection, secondary graft inflammation causing tissue fibrosis, graft contractures, and possibility of allergic reactions [1070,1181-1184].
Postoperative penile rehabilitation to improve surgical outcomes has been suggested with a number of studies describing the use of VED and PTT to prevent penile length loss of up to 1.5cm [1185]. Daily nocturnal administration of PDE5I enhances nocturnal erections, encourages perfusion of the graft, and may minimize postoperative ED rates [1186]. Massages and stretching of the penis have also been recommended once wound healing is complete.
Table 8.3: Results of tunical lengthening procedures for Peyronie’s Disease (data from different, non-comparable studies)
| Year of publication | No. of patients / studies | Success (%)* | Penile shortening (%)* | De novo ED (%)* | Follow-up (mo)* | |
| Autologous grafts | ||||||
| Dermis | 1974-2019 | 718 / 12 | 81.2% (60-100) | 59.9% (40-75) | 20.5% (7-67) | (6-180) |
| Vein grafts | 1995-2019 1995-2022 | 690 / 17 761 / 18 | 85.6% 85.8% (67-100) | 32.7% 29.8% (0-100) | 14.8% 14.2% (0-37) | (12-120) |
| Tunica albuginea | 2000-2012 | 56 / 3 | 85.2% (75-90) | 16.3% (13-18) | 17.8% (0-24) | (6-41) |
| Tunica vaginalis | 1980-2016 1980-2024 | 76 / 5 99 / 6 | 86.2% 88.1% (66-100) | 32.2% 18.6% (0-83) | 9.6% 11.2% (0-41) | (12-60) |
| Temporalis fascia / Fascia lata | 1991-2004 1991-2022 | 24 / 2 46 / 3 | 100% 95.6% (91-100) | 0% 13% (0-27) | 0% 15.2% (0-31.8) | (3-10) (3-19.3) |
| Buccal mucosa / Lingual mucosa | 2005-2016 2005-2024 | 137 / 7 204 / 9 | 94.1% 94.2% (88-100) | 15.2% 8.3% (0-80) | 5.3% 4.9% (0-10) | (12-45) (12-62) |
| Allografts (cadaveric) | ||||||
| Pericardium | 2001-2011 2001-2024 | 190 / 5 463 / 7 | 93.1% 85.1% (56-100) | 23.1% 22.1% (0-33) | 37.8% 18.5% (30-63) (4.5-63) | (6-58) |
| Fascia lata | 2006 | 14 / 1 | 78.6% | 28.6% | 7.1% | 31 |
| Dura matter | 1988-2002 | 57 / 2 | 87.5% | 30% | 17.4% (15-23) | (42-66) |
| Xenografts | ||||||
| Porcine SIS | 2007-2018 | 429 / 10 | 83.9% (54-91) | 19.6% (0-66) | 21.9% (7-54) | (9-75) |
| Bovine pericardium | 2002-2020 | 318 / 6 | 87.4% (76.5-100) | 20.1% (0-79.4) | 26.5% (0-50) | (14-67) |
| Bovine dermis | 2016 | 28 / 1 | 93% | 0% | 25% | 32 |
| Porcine dermis | 2020 | 19 / 1 | 73.7% | 78.9% | 63% | 85 |
| TachoSil® | 2002-2020 2002-2025 | 529 / 7 740 / 10 | 92.6% 90.2% (83.3-97.5) (80.6-97.5) | 13.4% 12.6% (0-93) | 13% 16.8% (0-21) (0-38.6) | (0-63) |
*Data are expressed as weighted average. Ranges are in parentheses.
ED = erectile dysfunction; SIS = small intestinal submucosa.
There have been no RCTs comparing surgical outcomes in PD. The risk of ED appears greater for penile lengthening procedures [951]. Recurrent curvature is likely to result from operating before the disease has stabilised, reactivation of the condition after stabilisation, or the use of early, re-absorbable sutures (e.g. Vicryl) that lose tensile strength before ensuing fibrosis provides adequate reinforcement of the repair. Accordingly, it is recommended that only non-absorbable sutures or slowly re-absorbed absorbable sutures (e.g. polydioxanone) should be used. With non-absorbable sutures, the knot should be buried to avoid troublesome irritation of the penile skin. This issue may be alleviated by the use of slowly re-absorbable sutures (e.g. polydioxanone) [1198]. Penile numbness is a potential risk of any surgical procedure involving mobilisation of the dorsal neurovascular bundle. This is usually a temporary neuropraxia due to bruising of the dorsal sensory nerves. Given that the usual deformity is a dorsal deformity, the procedure most likely to induce this complication is a lengthening (grafting) procedure, or the association with (albeit rare) ventral curvature [1059].
8.2.3.b.3. Penile prosthesis
Penile prosthesis implantation is typically reserved for the treatment of PD in patients with concomitant ED not responding to conventional medical therapy (PDE5I or intracavernous injections of vasoactive agents) [951]. Although inflatable prostheses have been considered more effective in the general population with ED, some studies support the use of malleable prostheses in these patients with similar satisfaction rates
[951,1199,1200]. The evidence suggests that there is no real difference between the available inflatable prostheses [1201]. Surgeons can and should advise on which type of prosthesis best suits their patient, but it is the patient who should ultimately choose the prosthesis to be implanted [1202].
Most patients with mild-to-moderate curvature can expect an excellent outcome simply by cylinder insertion [1136,1203]. If the intra-operative curvature after placement of the prosthesis is < 30° no further action is indicated, since the prosthesis itself will act as an internal tissue expander to correct the curvature during the subsequent six to nine months. If the curvature is > 30°, manual modelling may be proposed as a first-line treatment approach with the prosthesis maximally inflated (manually bent on the opposite side of the curvature for 90 seconds, often accompanied by an audible crack), although the supporting evidence is limited [1204-1206]. If a deviation > 30° persists after performing this manoeuvre, correction should be performed through shortening or lengthening procedures (incision with or without grafting) [1207-1212].
If it is larger, the defect may be covered using grafts commonly used in grafting surgery (described above) that prevent herniation and recurrent deformity or buckling due to scarring [1213,1214]. The risk of complications (infection, malformation, etc.) is not increased compared to that in the general population. A small risk of urethral perforation (3%) has been reported in patients with ‘modelling’ over the inflated prosthesis [1204].
In selected cases of end-stage PD with ED and significant penile shortening, a lengthening procedure, which involves simultaneous penile prosthesis implantation and penile length restoration, such as the 'sliding-' technique, has been proposed [1215]. However, the “sliding” technique is not recommended due to reported cases of glans necrosis because of the concomitant release of the neurovascular bundle and urethra, new approaches for these patients have been described, such as the MoST (Modified Sliding Technique), MuST (Multiple-Slit Technique) or MIT (Multiple-Incision Technique) techniques, but these should only be used by experienced high-volume surgeons and after full patient counselling [1216-1219].
While patient satisfaction after inflatable prostheses placement in the general population is high, satisfaction rates have been found to be significantly lower in those with PD. Despite this, depression rates decreased after surgery in PD patients (from 19.3%-10.9%) [1220]. The main cause of dissatisfaction after inflatable prostheses in the general population is shortening; therefore, these patients must be counselled that the prostheses are not designed to restore previous penile length [1220,1221].
In certain cases of PD (mostly complex deformities), plaque incision with grafting procedures performed without concomitant PPI may significantly increase the risk of postoperative complication, including ED (see Table 8.3). Consequently, primary PPI may represent an alternative, with high risk of complications, and the current evidence for this approach is limited [1222].
8.2.3.b.4. Summary of evidence and recommendations for surgical treatment of Peyronie’s disease
| Summary of evidence | LE |
| Surgery for PD should only be offered in patients with stable disease and with functional impairment. | 2b |
| In patients with concomitant PD and ED without response to medical treatment, PPI with or without additional straightening manoeuvres is the technique of choice. | 2a |
| In other cases, factors such as penile length, rigidity of erection, degree of curvature, presence of complex deformities and patient choice must be considered when deciding whether to undertake tunical shortening or lengthening procedures. | 3 |
| Recommendation | Strength rating |
| Perform surgery only when Peyronie’s disease (PD) is stable and sexual intercourse is compromised due to the deformity. | Strong |
| Assess penile length, curvature severity, erectile function (EF) (including response to pharmacotherapy in case of erectile dysfunction [ED]) and patient expectations prior to surgery. | Strong |
| Use tunical shortening procedures as the first treatment option for PD patients with adequate penile length and rigidity, less-severe curvatures, and absence of complex deformities (hourglass or hinge). The type of procedure used is dependent on surgeon and patient preference, as no procedure has proven superior to its counterparts. | Weak |
| Use tunical lengthening procedures for patients with PD and normal EF, without adequate penile length, severe curvature or presence of complex deformities. The type of graft used is dependent on the surgeon and patient preference, as no graft has proven superior to its counterparts. | Weak |
| Do not use the sliding technique as there is a significant risk of life changing complications (e.g. glans necrosis). | Strong |
| Use penile prosthesis implantation, with or without any additional straightening procedures (modelling, plication, incision or excision with or without grafting), in PD patients with ED not responding to pharmacotherapy. | Strong |
Figure 8.1: Treatment algorithm for Peyronie’s disease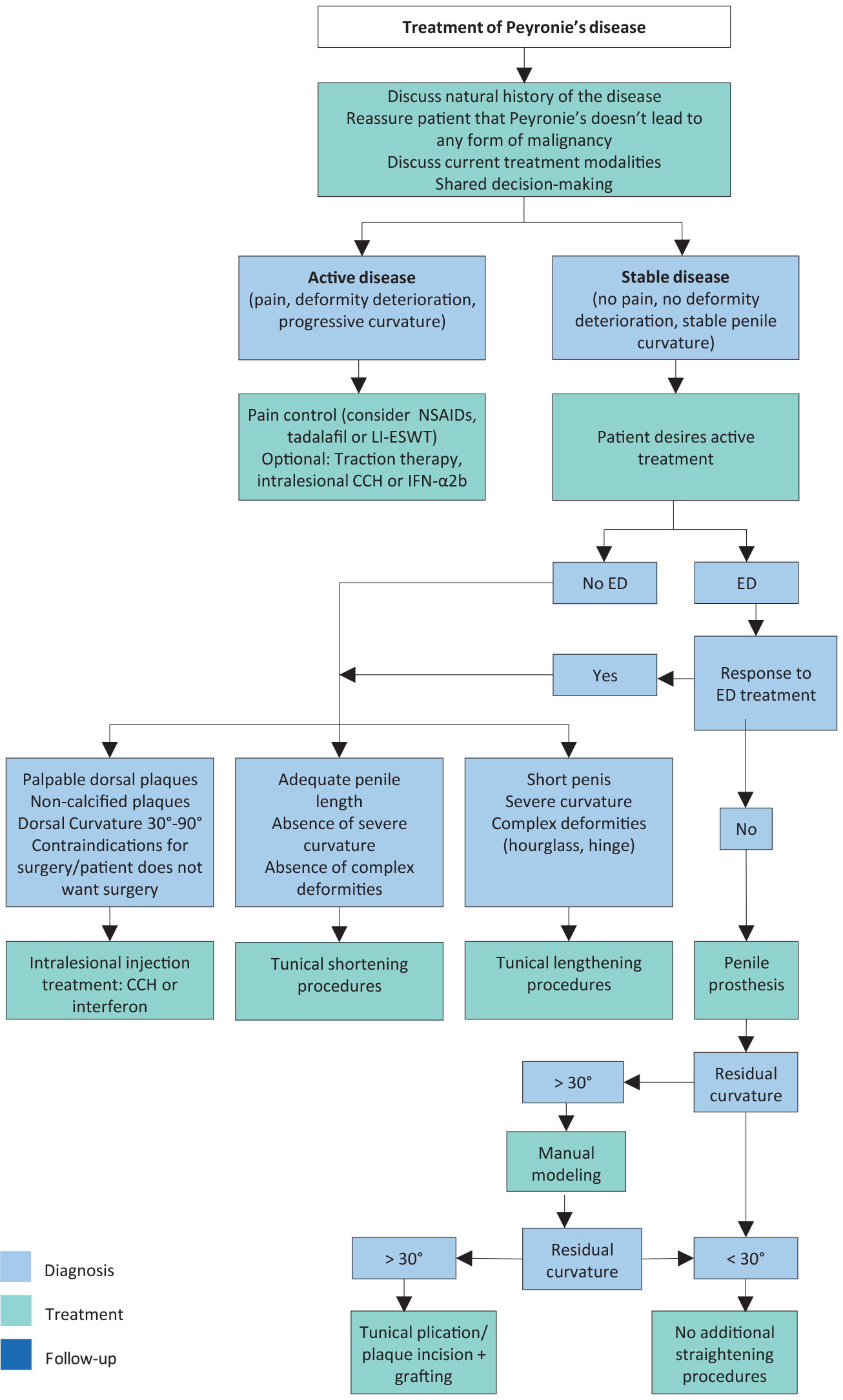
CCH = collagenase clostridium histolyticum; ED = erectile dysfunction; IFN-α2b = interferon-α2b; LI-ESWT = low-intensity extracorporeal shockwave treatment; NSAIDs = non-steroidal anti-inflammatory drugs.