
9. PENILE SIZE ABNORMALITIES AND DYSMORPHOPHOBIA
9.1. Definition, epidemiology and classification
9.1.1. History
Throughout history, the size of the penis has symbolised a marker of masculinity [1223] and has created intense debate in societies with different social and cultural implications [1224]. Along with the capacity for vaginal penetration, the penis is linked to an ancestral sense of male fertility and sexual performance, making the size of the penis a distinguishing male identity [1225,1226]. Claims of male supremacy and dominance as represented by phallometric designs can be found across cultures and history, and is still supported by contemporary media, including the pornographic industry [1227,1228].
Overall, cosmetic surgery has the potential to restore self-esteem, reduce anxiety, social phobia and depressive mood states regarding body concerns, increasing well-being and QoL [1229,1230]. Yet, some candidates for cosmetic surgery may have psychopathological conditions and surgery may result in negative outcomes
[1230,1231].
In the real-life setting, 84% of females report being satisfied with their male partner’s penile size, whereas only 55% of male partners were satisfied with their penile size and 45% reported that they would like to have a larger penis [1232]. In this context, men with a high level of social-desirability were more likely than others to self-report having a larger penis [1233]. A study also demonstrated that reducing the depth of penetration led to a statistically significant 18% reduction of overall sexual pleasure with an average 15% reduction in length of the penis [1234].
The subjective impression of penile size may have a negative effect on sexual functioning and QoL, impacting sexual life in about 10% of men [1235-1237]. This prevalence sharply rises in patients seeking penile augmentation procedures [1238,1239].
Furthermore, the fact that a subgroup of men do not achieve reasonable levels of satisfaction or emotional adjustment after penile augmentation procedures underlines that, with certain psychopathological conditions, they will not benefit from such invasive procedures [1240]. These men may represent a psychologically vulnerable group of individuals in whom penile augmentation procedures will have negative effects and, as such, require clinical and psychological support. Clinicians should anticipate and address such vulnerability through a tailored psychological evaluation and further consider cultural standards, enabling an understanding of patient expectations [1241].
With the increased use of penile augmentation procedures worldwide, either medical or surgical, it becomes crucial to create evidence-based recommendations to guide clinicians in this challenging and controversial area.
9.1.2. Definition
To date, short penis condition represents both a diagnostic and treatment challenge [1242,1243]. An accurate measurement of the penile shaft is a mandatory step in the assessment of patients complaining of a short penis and defining the norm [1244]. A standard tool to address penile measurements and to counsel patients seeking penile augmentation procedures is needed. To date, the standard penile size has yet to be clearly defined. Even though several investigators have attempted to provide objective measurements to define a normal penile size, there is no consensus on this (See Table S9.1 in Appendix 5 of the online supplementary evidence).
The other factor that strongly affects penile measurements is the interobserver variability and underestimation of the SPL when compared to the erect state [1245].
Despite these limitations, SPL – defined as the distance between the pubic symphysis and the apex of the glans – represents the most overlapping measurement of the erect penis. Accordingly, an SPL of less than 2.5cm standard deviations below the mean for the male’s age and race is considered to be micropenis [1246,1247].
| Summary of evidence | LE |
| There is a difference between true micropenis (anatomical-endocrinological), short penis (complaint) and buried penis (complaint short penis + obesity) (Panel consensus). | 4 |
| Small penis anxiety/syndrome refers to a man’s excessive anxiety regarding his normal-sized penis. | 3 |
| A true micropenis is a congenital condition where the SPL is 2.5cm standard deviations less than the average length in the population group and is the result of an underlying genetic or endocrine condition. | 3 |
| A buried penis is a normal sized penis where there is functional and visible loss of penile length due to an underlying pathological condition, such as obesity or traumatic loss of length. The penis is covered by prepubic, scrotal or penile subcutaneous tissue or skin. | 3 |
| Penile dysmorphic disorder is a shorthand concept applied to body dysmorphic disorder cases characterised by a strong focus on a perceived deficiency or flaw in a normal size or shape penis, resulting in mental health impairment and significant damage in important areas of the individual’s life. | 3 |
9.1.3. Epidemiology and classification
The overall incidence of micropenis in the male population is not clearly documented. Epidemiological studies demonstrate that between 0.015-0.66% of male newborns have a micropenis [1248,1249]. There are concerns that the prevalence of this congenital abnormality is increasing due to in utero exposure to endocrine-disrupting chemicals before and during pregnancy [1249]. Despite the limited prevalence of micropenis, there is a major demand for penile augmentation procedures worldwide. This phenomenon can be partially explained by an increased interest in pornography and the altered perception of a normal penile size [1224,1250,1251].
Due to the heterogeneity of clinical situations related to short penis conditions, a classification based on the underlying aetiology is provided below (Table 9.1).
Table 9.1: Classification of the clinical conditions underlying a short penis condition or dysmorphophobia in adults
| Group name | Aetiology | Definition | Pathogenesis | Prevalence, % |
| False penile shortness | Acquired | Reduced exposure of the penile shaft in the presence of normal penile size | Adult acquired buried penis | N/A |
| Intrinsic penile shortness | Congenital | Small penis due to an incomplete genital development secondary to a congenital condition |
| 0.9-2.1 |
| Intrinsic penile shortness | Acquired | Shortening/shrinking of the corpora cavernosa due to an acquired pathological process |
| N/A |
| Body dysmorphic disorder | Acquired | Perceived defect or flaw in the individual’s physical appearance followed by significant distress or impairment in important areas of the individual’s life |
| 1.8-9.5 |
PP = penile prosthesis.
9.1.3.a. False penile shortness – congenital or acquired
Among causes underlying a false penile shortness, the buried penis is the only well-known condition. Historically, buried penis has been considered a congenital disease affecting children: the so-called 'concealed penis' or 'webbed penis' [1252,1253]. Indeed, an abnormal development of the dartos fascia may lead to the entrapment of the penile shaft to the peri-genital tissue leading to this clinical manifestation. On the other hand, buried penis in an adult is widely recognised as an acquired condition, termed adult acquired buried penis (AABP) [1254].
The aetiology underlying the development of AABP is deemed to be related to a chronic inflammatory state of the penile dartos which leads to a progressive retraction and scarring of the peri-genital teguments [1255,1256]. The progressive entrapment of the phallus causes a moist environment which facilitates bacterial and fungal growth causing chronic inflammation [1257]. The ensuing fibrosis results in further entrapment of the penile shaft in the peri-genital tissue [1256,1257].
Although the exact prevalence of AABP is unknown, its incidence seems to be increasing along with the growing prevalence of obesity, which represents the main risk factor [1258]. Other factors contributing to AABP include aggressive circumcision, following surgical treatment in the obese or penile cancer, or chronic dermatological conditions such as lichen sclerosis [1259].
The AABP is commonly associated with erectile and voiding dysfunctions, difficulties in maintaining adequate genital hygiene and a poor QoL [1259-1261]. A summary of risk factors for AABP and underlying issues requiring surgery is detailed in Table S9.2 in Appendix 5 of the online supplementary evidence.
The aim of AABP treatment is to restore the functional genital anatomy and improve QoL [1259,1260]. So far, different authors have proposed several classifications for AABP based upon both clinical presentation and the surgical procedure required [1254,1262].
9.1.3.b. Intrinsic penile shortness – congenital
This category encompasses the so-called 'true micropenis' [1263-1265]. Despite male genital malformations being recognised as the most common birth defects, they represent a rare clinical entity with a prevalence between 0.9% and 2.1% [1266,1267]. Normal genital development is under the influence of hormonal stimulation during the foetal and pubertal periods [1268]. Several genetic syndromes may cause disturbance of the physiological hormonal axis needed for a normal genital development [1263,1269]. In up to 25% of cases, micropenis may also exist as an isolated finding without a definitive etiological cause. The classification of the clinical conditions associated with intrinsic penile shortness in adults is presented in Table 9.2.
Table 9.2: Classification of the clinical conditions underlying intrinsic penile shortness in adults
| Aetiology | Underlying causes |
| Hypogonadotropic hypogonadism |
|
| Hypergonadotropic hypogonadism |
|
| Syndromic or multiple congenital anomalies |
|
| Unknown | - |
Amongst the pre-existing clinical entities associated with micropenis, the bladder exstrophy-epispadias complex is the most studied [1259,1260,1265]. It represents a spectrum of genitourinary malformations ranging in severity from epispadias to bladder exstrophy or exstrophy of the cloaca. It is considered as a rare disease, with a prevalence at birth of 1/10,000 [1263,1265,1267,1270]. Even though surgical reconstruction aims to improve body image, this clinical entity is frequently burdened by psychosocial and psychosexual dysfunctions in the long term [1271-1277]. Additionally, male infertility is frequently associated due to poor sperm quantity or quality and hormonal impairment [1278].
9.1.3.c. Intrinsic penile shortness – acquired
This category includes a series of pathological entities that lead to the shortening of the corpora cavernosa. The different aetiologies are classified in Table 9.2. The mechanism underlying intrinsic penile shortening is acute, as in cases of penile trauma or surgical amputation for penile cancer, or chronic, due to a progressive fibrotic process involving the corpora cavernosa [1279-1281].
Traumatic genital injuries may commonly result from traffic accidents and gunshot wounds [1281]. Rarely, a penile amputation is the result of circumcision or genital surgical procedures such as hypospadias repair, PPI or urethroplasty, and may result in a decrease in penile length [1282-1286].
Among chronic causes of penile shortening, PD, treatments for PCa, particularly RP and radical cystectomy, represent the most common [1238,1279,1280,1287-1295].
9.1.3.d. Body dysmorphic disorder
Body dysmorphic disorder (BDD) is a clinical diagnosis defined by the APA DSM-5 as the strong distress generated by perceived defect(s) or flaw(s) in the individual’s physical appearance. This flaw is not observable to others, or, in case it exists, it appears only slightly [1296]. This condition is followed by significant impairment in important areas of the individual’s social or occupational life. Body dysmorphic disorder has been allocated to the Obsessive Compulsive and Related Disorders section [1296]. Muscle dysmorphia is a typology within BDD characterising individuals – usually men – with a strong preoccupation with their perceived small muscles and body shape. Sometimes, men with BDD/muscle dysmorphia also present with an exaggerated focus on the size or shape of their penis. In those cases, penile dysmorphic disorder (PDD) can be used as a shorthand concept – not listed in APA’s DSM-5 coding system. Both BDD and PDD are conceptually different from small penis anxiety (SPA) or small penis syndrome, which refers to a man’s excessive anxiety regarding their normal-sized penis. Small penis anxiety is not included under APA’s classification, but men with SPA may be at risk for BDD [1297]. All these definitions exclude men with true micropenis [1296,1298,1299]. Prevalence data show that 2.2% of men in the USA and 1.8% in Germany suffer from BDD [1296]. Between 3-16% of patients undergoing cosmetic surgery are expected to present with BDD, a higher rate in men (15.3%) than in women (10.9%) [1300].
These psychopathological entities must be differentiated from gender dysphoria, which is the clinical distress associated with incongruence between gender identity and the gender assigned at birth, and from Koro, which is the sudden anxiety that the penis will retract into the abdomen [1296].
9.1.4. Summary of evidence and recommendations for classification of short penile size
| Summary of evidence | LE |
| Male genital malformations represent a rare clinical entity with an overall prevalence between 0.9% and 2.1%. | 3 |
| Obesity, lichen sclerosis and penile cancer treatment are risk factors for AABP. | 4 |
| The AABP is commonly associated with erectile and voiding dysfunctions, difficulties in maintaining adequate genital hygiene and a poor QoL. | 3 |
| The AABP can be staged upon both clinical presentation and the surgical procedure required according to available classification systems. | 3 |
| Bladder exstrophy-epispadias complex is a rare clinical condition frequently associated with male genital malformations, particularly micropenis. | 2b |
| Penile traumatic or surgical amputation due to penile cancer are the most common acute causes of intrinsic penile shortening. | 3 |
| The most frequent aetiologies leading to a chronic intrinsic penile shortening are PD, treatments for PCa (RP, radiation therapy and androgen-deprivation therapy) and radical cystectomy. | 2b |
| Body dysmorphic disorder is a clinical entity associated with a significant distress or impairment in important areas of the individual’s life. | 2b |
| Penile dysmorphic disorder can be used as a shorthand concept to describe BDD patients mainly focused on penile size/shape. | 4 |
| Body dysmorphic disorder/PDD can be revealed in patients requiring cosmetic surgery. | 3 |
| Recommendations | Strength rating |
| Perform a detailed genital examination should be considered in all males and particularly in males with body mass index > 30, lichen sclerosis or penile cancer history and complaints of urinary/sexual difficulties or poor cosmesis to exclude the presence of adult acquired buried penis (AABP) condition. | Strong |
| Use classification systems to classify AABP clinical presentation and surgical management. | Weak |
| Inquire on the presence of body dysmorphic disorder/penile dysmorphic disorder in patients with normal-sized penis complaining of short penile size. | Strong |
9.2. Diagnosis
9.2.1. Medical history, physical examination and psychological assessment
9.2.1.a. Medical history
The first step in the evaluation of short penis is a detailed medical history [1301]. Common causes of penile shortness should be screened and observed (e.g. history of phimosis, priapism, hypospadias/epispadias, penile trauma, penile cancer, PCa, and penile pain with or without acquired penile curvature suggestive of PD). A past or present diagnosis of BDD should also be noted.
9.2.1.b. Sexual history
Besides a comprehensive clinical interview with open questions regarding sexual education, development or previous sexual experiences and fantasies, psychometric tools can be used. These include measurements of sexual functioning (e.g. IIEF), sexual distress (e.g. The Sexual Distress Scale for men), and sexual satisfaction (e.g. Global Measure of Sexual Satisfaction) [323,1302,1303]. The propensities for sexual excitation and sexual inhibition may be further considered (e.g. Sexual Inhibition/Sexual Excitation Scales), as well as measurements of relationship satisfaction (e.g. Global Measure of Relationship Satisfaction) [1303,1304]. Special focus should be put on the assessment of sexual performance expectations (e.g. The Dysfunctional Sexual Beliefs Questionnaire) [1305]. As a complementary assessment, body image perception can be further considered (e.g. The Body-Image Questionnaire).
9.2.1.c. Physical examination and penile size measurements
An accurate physical examination focused on the genital area is essential to the patient's initial assessment. The assessment of penile size and shape is mandatory to plan any subsequent medical or surgical treatment, but methods for penile measurements seem to vary amongst surgeons [1244,1306]. The Panel considers a stretch penile length measurement as the bare minimum. If possible, the Panel also advocates additional measurements in both flaccid and erect state after intracavernosal injection of erectogenic agents, compulsory before any surgical indication. Stretched penile length can be measured both dorsally and/or ventrally from the penopubic skin junction-to-glans tip (STT) or dorsally from the pubic bone-to-glans tip (BTT) using either a measuring tape or a Vernier calliper. The measurement of penile size has not been standardised, and no consensus definition exists because of high heterogeneity in data assessment and reporting methodologies across studies [1306].
Penile girth should be noted in every patient, and both distal (coronal) and mid-shaft measurements should be recorded. Both measures of circumference can be compared to the head-to-base ratio. The former can help classify penile shape, which can be documented through photography [1307]. Although used as a surrogate, STT clearly underestimates erect penile length by about 20% [956,1308]. Bone-to-glans tip appears to have a better correlation with erect penile length, especially in males that are overweight or obese [956].
Table 9.3: Penile size measurement
| Penile size measurement |
| Length |
| State: Erect, stretched or flaccid Anatomic landmarks Dorsal and/or ventrally from the penopubic skin junction-to-glans tip Dorsally from the pubic bone-to-glans tip |
| Girth |
| State: Erect or flaccid Anatomic landmarks Proximal (penopubic skin junction) Middle shaft Distal (Coronal or subcoronal) |
| Shape |
| Head-to-base ratio Standardised photography |
9.2.1.d. Psychological assessment
A subgroup of men requesting penile augmentation procedures, usually surgery, present with strong psychological vulnerability, including BDD [1297]. This subgroup of men may be at risk for increasing psychopathology and suicide attempts and are unlikely to achieve their expectations of surgery [1309]. There is a set of freely available self-reported tools that may be used to screen patients at risk for psychopathology or poor surgical outcomes, including the Body Dysmorphic Disorder Questionnaire and The Cosmetic Procedure Screening Scale for Penile Dysmorphic Disorder, screening for psychopathological cases regarding BDD and PDD [1297,1310]. Likewise, The Male Genital Self-Image Scale, and the Index of Male Genital Image, measuring men’s perceptions and satisfaction regarding their genitals [1311,1312]. In addition, the Beliefs About Penile Size (BAPS) captures beliefs about the size of the penis as well as internal psychological processes [1313]. Evidence on BDD/PDD, further psychopathological comorbidities, and the differential diagnosis regarding personality disorders, and disorders from the obsessive-compulsive, psychotic, or emotional spectrum, should be performed by an accredited mental health expert. In addition, the subjective penile size perception should be evaluated [1240].
9.2.1.e. Counselling and outcomes assessment - Validated questionnaires
The Augmentation Phalloplasty Patient Selection and Satisfaction Inventory (APPSSI) questionnaire is a five-item questionnaire proposed for the assessment and counselling about penile augmentation surgical treatment [1314]. The BAPS is a ten-item questionnaire created for audit and outcome research to assess men’s beliefs about penile size [1313]. Both questionnaires have failed to correlate with penile size and lack of objective validation has restricted their use.
Other well-known self-reported psychosexual questionnaires may be considered: the IIEF-15 and the MSHQ should be administered to record baseline sexual function status and can also be used to assess its changes after treatment; the Erectile Dysfunction Inventory of Treatment Satisfaction (EDITS) can also be helpful to assess patient and partner's treatment satisfaction [323,1315,1316].
9.2.2. Imaging
There is a lack of evidence regarding the use of imaging techniques in the assessment of patients complaining about penile shortness. Although a penile Doppler US or MRI may provide additional data on penile anatomy and the extent of penile burying, there is no evidence that this additional information contributes to the physical examination to justify its routine use in this clinical scenario [1244,1317-1320].
| Summary of evidence | LE |
| Medical/sexual history taking and physical examination are essential parts of the evaluation of males with a short penis complaint. | 4 |
| Among stretched penile measurements, STT may underestimate erect penile length. | 2b |
| Among stretched penile measurements, BTT has a better correlation with erect penile length, especially in males that are overweight or obese. | 2b |
| Flaccid and erect state measurements to assess penile length may add useful information on penile size. | 4 |
| Penile girth assessment may add useful information on penile size and shape. | 4 |
| The Body Dysmorphic Disorder Questionnaire, The Cosmetic Procedure Screening Scale for Penile Dysmorphic Disorder, The Male Genital Self-Image Scale and the Index of Male Genital Image are self-reported tools useful to screen patients at risk for psychopathology. | 2b |
| Mental health counselling is helpful in detecting males requesting penile augmentation procedures present with strong psychological vulnerability, including BDD/PDD. | 2b |
| Validated questionnaire (e.g. APPSSI, BAPS, IIEF-15, MSHQ, EDITS) are helpful in assessing baseline sexual function and beliefs about penile size. | 4 |
| Recommendations | Strength rating |
| Take a comprehensive medical and sexual history in every patient presenting with a complaint of short penile size. | Strong |
| Use stretched penile measurements (skin junction-to-glans tip or dorsally from the pubic bone-to-glans tip) to define penile length. | Weak |
| Measure flaccid and erect measurements to assess penile length in detail. | Weak |
| Measure penile girth in every patient presenting complaining of a short penile size. | Weak |
| Use validated questionnaires to screen for body dysmorphic disorder (BDD) in cases of a normal-sized penis. | Weak |
| Use validated questionnaires (e.g. IIEF-15, BAPS) to assess baseline sexual function and beliefs concerning penile size. | Weak |
| Refer patients with suspected BDD for mental health counselling. | Strong |
9.3. Management
9.3.1. Non-surgical treatments
9.3.1.a. Psychotherapy
Penile augmentation is often motivated by the desire to improve self-perception and self-esteem [1321]. Cosmetic treatments may help increase individuals’ well-being and QoL, improving self-esteem and emotional states [1229,1230,1244]. Psychotherapy is recommended when psychopathological comorbidities are detected or when aversive relationship dynamics may underlie the request for penile augmentation. Addressing the motivations and expectations of patients and their partners regarding penile augmentation appears to be a key psychotherapeutic target, as no other empirical evidence is available. Similarly, males with BDD and SPA present with a significant discrepancy between the perceived and ideal size of the penis, internalising the belief that they should have a larger penis [1322]. Cognitive behaviour therapy for BDD could be applied to cases of anxiety regarding penis size, although no clinical trials have been reported [1323]. Psychotherapy may normalise the great variability of genital shape and size [1239]. Managing patient expectations may help improve surgical outcomes and overall well-being.
9.3.1.b. Penile traction therapy
Despite the various surgical techniques, there are also non-invasive methods that are used to enhance penile length, including PTT [1324]. In a pilot phase-II prospective study that evaluated the efficacy and tolerability of a penile-extender device in the treatment of short penis, Gontero et al., used the same traction device for at least four hours per day for six months and achieved a significant gain in length, of +2.3 and +1.7cm for the flaccid and stretched penis, respectively (both p < 0.001) [1325]. However, the change in the penile girth was not significant. In a further prospective study, these results were confirmed by Nikoobakht et al., who found a significant improvement in the mean length both for the flaccid (8.8 ± 1.2cm to 10.5 ± 1.2cm, P < 0.05) and the stretched state (11.5 ± 1.0cm to 13.2 ± 1.4cm, p < 0.05) following three months of use of a penile traction device [1326]. At six-month follow-up, compared to baseline, a mean gain of +1.7 ± 0.8, +1.3 ± 0.4, and +1.2 ± 0.4cm was reported for the flaccid, stretched, and erect penile lengths, respectively (p < 0.001, for all). The broad spectrum of available PTT studies is summarised in Table 9.4.
Overall, PTT seems effective in lengthening the penis both in the flaccid and stretched state, with minimal side effects. It is not effective for penile girth enhancement. The quality of evidence is poor due to the lack of RCTs, and the availability of only heterogenous and small cohorts. Penile traction therapy has proved effective in the restoration of length or correction of deformities due to several diseases, including PD or post-RP conditions [536,1038,1327,1328].
Table 9.4: Penile traction therapy
| Penile traction therapy | ||||||
| Author | n | Study design | Device | Treatment protocol | Mean age ± SD | Mean gain in penile dimensions cm (SD) |
| Nowroozi et al. [1329] | 54 | Prospective | AndroPenis | 4-6 hours per day for 6 months | 30.1 ± 4.8 | Flaccid length: 1.7 ± 0.8 Stretched length: 1.3 ± 0.4 Erected length: 1.2 ± 0.4 |
| Nikoobakht et al. [1326] | 23 | Prospective | Golden Erect | 4–6 hours per day during the first 2 weeks and then 9 hours per day until the end of the third month | 26.5 ± 8.1 | Flaccid length:1.7 Stretched length: 1.71 Circumference: -0.22 Glans penis circumference: -0.35 |
| Gontero et al. [1325] | 21 | Prospective | Golden Erect | at least 4 h/day for 6 months | 45.7 ± 11.1 | Flaccid length: 2.3 Stretched length: 1.7 Circumference: NR |
NR = not reported; SD = standard deviation.
9.3.1.c. Vacuum erection device
Vacuum erection devices are generally considered for patients who fail oral ED therapies [457,1301]. Data regarding the use of VEDs on penile elongation is scarce. In a study with 27 males whose SPL was < 10cm, the use of a VED three times a week for 20 minutes on each occasion, for six months, did not result in a significant increase in flaccid or SPL [1330]. The benefits of using VED following PPI and RP have been demonstrated in the literature [1330-1335].
9.3.1.d. Endocrinological therapies
For a long time, testosterone administration has been to increase the length of the penis in infant or pre-pubertal children with micropenis. Topical administration of T or DHT has also been proposed, with better outcomes reported with DHT, especially in poor responders to T or in those with type 2 alpha reductase deficiency [1336,1337]. The possible use of a combination of hCG and FSH treatment has also been proposed, with positive outcomes [1338,1339]. Despite the suggested treatment, no face-to-face comparisons are available so far.
9.3.1.e. Summary of evidence and recommendations for the non-surgical management of short penile size
| Summary of evidence | LE |
| Psychotherapy should not be undertaken in the realm of preventing individuals’ legitimate choice to improve their lives. Conversely, psychotherapy is recommended when psychopathological comorbidities are detected, or when aversive relationship dynamics may underlie the request for penile augmentation. | 3 |
| Cognitive behaviour therapy for BDD could be applied to cases of anxiety regarding penis size. | 3 |
| Penile traction therapy is an effective treatment to achieve penile lengthening. | 3 |
| Vacuum erection devices is an ineffective treatment in achieving penile lengthening. | 3 |
| Testosterone therapy, transdermal DHT and recombinant gonadotropins can restore penile size in boys with micropenis or disorders of sex development. | 2b |
| Testosterone therapy does not increase penile size in adult males and in males with LOH. | 3 |
| Recommendations | Strength rating |
| Consider psychotherapy when psychopathological comorbidities are detected, or when aversive relationship dynamics may underlie the request for penile augmentation. | Strong |
| Consider the use of penile traction therapy as a conservative treatment to increase penile length. | Weak |
| Consider the use of vacuum erection devises to increase penile length. | Weak |
| Use endocrinological therapies to restore penile size in male children with micropenis or disorders of sex development. | Strong |
| Do not use testosterone therapy or other hormonal therapies to increase penile size in males after puberty. | Strong |
9.3.2. Surgical treatments
9.3.2.a. Surgical treatment of adult acquired buried penis
9.3.2.a.1. Adult acquired buried penis surgical procedures classification
According to the classification proposed by Pariser et al., different procedures may range from low complexity (including un-burying of penile shaft, reconstruction of penile shaft with the use of skin flaps or grafts, plastic surgical techniques to reconstruct the scrotum) to high complexity (including surgical removal of the suprapubic fat pad [escutcheonectomy] and operations to skin and subcutaneous fat layers of the abdominal wall [apronectomy]) [1262].
The purpose of any surgical approach is to unbury the penile shaft, reconstruct genital teguments and eventually remove peri-genital or excess abdominal tissue to reduce the risk of recurrence. The goal is to balance an effective surgical procedure aiming to improve patient QoL, while minimising the incidence of postoperative complications. Lifestyle changes and risk factors modification, particularly weight loss, are widely considered as a proactive approach to minimise AABP surgical complications and should be encouraged before surgical intervention is undertaken. The broad spectrum of surgical interventions described to manage AABP is summarised in Table S9.3 in Appendix 5 of the online supplementary evidence. The current evidence highlights the efficacy of AABP surgical treatment which has a low incidence of recurrence and satisfactory functional outcomes, as shown in Table S9.4 in Appendix 5 of the online supplementary evidence, yet there is a significant incidence of postoperative complications (up to 3.5% of grade V according to Clavien-Dindo Classification) [1340].
| Summary of evidence | LE |
| Various surgical procedures may be considered to restore genital anatomy in AABP patients. | 3 |
| Acquired adult buried penis surgery is burdened by a significant incidence of postoperative complications. | 3 |
| Lifestyle changes and risk factors modification, particularly weight loss, are widely considered as a proactive approach to minimise AABP surgical complications. | 4 |
| Surgery for AABP may provide satisfactory functional outcomes with a low incidence of recurrence. | 3 |
| Recommendations | Strength rating |
| Extensively counsel patients on the benefits and complications of adult acquired buried penis (AABP) surgery. | Strong |
| Initiate lifestyle changes and modification of risk factors, particularly weight loss, to minimise AABP surgical complications and optimise surgical outcomes. | Strong |
| Consider surgical treatment to address AABP. | Weak |
9.3.2.b. Surgical treatment of congenital intrinsic penile shortness
Current literature reports a wide spectrum of possible surgical interventions aimed to address penile shortness. The proposed spectrum of surgical interventions starts from less invasive procedures – such as suspensory ligament release (SLR) – to more complex genital reconstruction - such as total phallic reconstruction (TPR) [1341,1342].
9.3.2.b.1. Suspensory ligament release
This technique involves a surgical incision and SLR of the penis, which attaches the penis to the pubic bone. The surgical access is via an infrapubic incision and may be combined with an elongating V-Y skin-plasty [1342]. Several authors reported outcomes of SLR in the context of a congenital intrinsic penile shortness (Table S9.5 online supplementary evidence Appendix 5).
Littara et al., conducted penile elongation in 21 patients, enlargement in 33 patients, and combined elongation and enlargement in 301 patients, respectively [1343]. The technique was based on penile lipofilling combined with V-Y infrapubic skin-plasty and SLR. At 12 months following the surgical procedure, length at rest significantly increased from 8.8cm to 11.4cm, SPL significantly increased from 12.4cm to 13.5cm, and circumference at rest significantly increased from 8.3cm to 11.06cm. The IIEF-5 also increased from 21.5 to 23. The outcomes of SLR are summarised in Table S9.5 in the online supplementary evidence and in Appendix 5.
9.3.2.b.2. Ventral phalloplasty/scrotoplasty
This intervention is based on a ventral shaft skin-plasty to move the penoscrotal angle proximally and increase the exposure of the penile shaft. A longitudinal incision or Z-plasty at the penoscrotal junction, securing of the tunica albuginea to the proximal tunica dartos was performed by Xu et al., in 41 patients [1344]. Correction was successful in all patients with an improved median length of + 2.1cm in the flaccid state.
9.3.2.b.3. Suprapubic lipoplasty/liposuction/lipectomy
This intervention aims to reduce the thickness of the suprapubic fat pad either with a minimally invasive approach (liposuction) or surgically (lipectomy). The flattening of suprapubic fat pad aims to increase penile shaft exposure.
Ghanem et al., performed liposuction in ten patients using a 50-cc syringe with a 3- and 6mm liposuction needle [1345]. The amount of fat removed ranged from 325 to 850mL with a mean of 495.50 ± 155.39mL. Three (30%) of the patients were very satisfied with the postoperative result, five (50%) patients were satisfied, one patient (10%) was neither satisfied nor dissatisfied, and one (10%) patient was dissatisfied. No patients were very dissatisfied. Shaeer’s monsplasty technique was investigated in 20 patients [1346]. At three months postoperatively, the flaccid visible length was 7.1 ± 2.1cm, with a 57.9% improvement in length, and erect visible length was 11.8 ± 2.1cm, with a 32% improvement in length. At final follow-up (18 months) a 73.1% improvement in satisfaction rate was detected.
9.3.2.b.4. Total phallic reconstruction
This represents the most complex genital reconstruction possible, aiming to create a new phallus with a neo-urethra. The operation is reserved for the severe penile insufficiency cases (e.g. congenital micropenis, exstrophy-epispadias complex) as benefit should be balanced over possible complications [1341].
Lumen et al., treated seven male patients (aged 15 to 42 years) with phalloplasty (six with radial forearm free flap and one with anterolateral thigh flap) and implant surgery was offered approximately one year after the phallic reconstruction [1347]. There were no complications after surgical formation of the neophallus. Two complications were reported in the early postoperative period. Two patients developed urinary complications (stricture and/or fistula). Patient satisfaction after surgery was high in six cases and moderate in one case. Four patients underwent penile implant surgery and 50% were subsequently removed.
Perovic et al., conducted TPR using musculocutaneous latissimus dorsi in 12 patients [1348]. The mean (range) follow-up was 31 (6–74) months, and the penile size was 16 (14–18) cm long and 13 (11–15) cm in circumference. There was no flap loss or partial skin necrosis.
Garaffa et al., reported a series of TPR using the radial artery forearm free flap in 16 patients with bladder/cloacal exstrophy and micropenis-epispadias complex [1349]. In one patient, the distal third of the phallus was lost due to acute thrombosis of the arterial anastomosis immediately postoperatively. Almost all (93%) were fully satisfied in terms of cosmesis and size. Urethral stricture and fistula were the most common complications, which developed only at the native neourethral anastomosis. They were successfully managed by revision surgery. Sexual intercourse was achieved in 11 of the 12 patients who underwent PPI.
9.3.2.b.5. Summary of evidence and recommendations for surgical treatment of congenital intrinsic penile shortness
| Summary of evidence | LE |
| Considering the wide spectrum and the complexity of surgical interventions aimed to address penile shortness, this surgery should be reserved to high volume centres. | 4 |
| Suspensory ligament release, ventral phalloplasty and suprapubic lipoplasty/liposuction/lipectomy provide an objective increase in penile length. | 3 |
| Suspensory ligament release, ventral phalloplasty and suprapubic lipoplasty/liposuction/lipectomy are associated with a significant incidence of complications. | 3 |
| Total phallic reconstruction provides satisfactory surgical and functional outcomes in males with micropenis. | 3 |
| Recommendations | Strength rating |
| Perform surgery for adult acquired buried penis (AABP) in high volume centres. | Strong |
| Use suspensory ligament release (SLR), ventral phalloplasty and suprapubic lipoplasty/liposuction/lipectomy to address penile lengthening. | Weak |
| Extensively discuss possible complications related to SLR, ventral phalloplasty and suprapubic lipoplasty/liposuction/lipectomy. | Strong |
| Use total phallic reconstruction to restore genital anatomy in patients affected by congenital micropenis. | Weak |
9.3.2.c. Surgical treatment of acquired penile shortness
9.3.2.c.1. Penile prosthesis implantation
The literature fails to show a direct relationship between PPI and penile length in men with ED and no concomitant PD. In a study by Deveci et al., SPL was evaluated in men undergoing primary implant surgery due to diabetes or RP [1350]. Either three-piece (Alpha-1, Mentor, USA) or two-piece implants (Ambicor, AMS, Boston Scientific, USA) were used and most patients (72%) reported a subjective decrease in penile length, although no statistically significant difference was demonstrated in measured SPL [1350]. In another study, 45 patients with PD with no deformity or penile curvature < 30° or severe penile fibrosis/scarring were implanted with an AMS 700 LGX [1351]. The mean SPL improved from 13.1 ± 1.2cm to 13.7 ± 1.1cm and 14.2 ± 1.2cm at six and 12 months, respectively. A significant difference was also observed in the length of the stretched flaccid penis between six and 12 months [1351]. Some authors have evaluated the erect penile length following PPI. In a prospective study where patients with PD were excluded, erect penile length was compared from baseline achieved by intracavernosal injection and after PPI inflation. The authors demonstrated that there were 0.83 ± 0.25cm, 0.75 ± 0.20cm and 0.74 ± 0.15cm decreases in erect penile length six weeks, six months, and one year postoperatively, respectively [1352]. A study where patients with PD were excluded confirmed these results as the median preoperative pharmacologically induced length (14.25 ± 2cm) was decreased to median post-prosthesis penile length (13.5 ± 2.13cm) [1353].
9.3.2.c.2. Penile disassembly
Penile disassembly has been described as a technique for penile lengthening [1354]. It basically consists of the separation of the penis into its anatomical components and inserting autologous cartilage to the space created between the glans cap and the tip of corpora cavernosa. Perovic et al., in a study with 19 patients submitted to penile disassembly and implantation of autologous rib cartilage followed by VED therapy, reported an increase of 3cm and 3.1cm in SPL and erect length, respectively [1354]. The results of this surgery are poorly documented and significant complications, such as glans necrosis, can ensue.
9.3.2.c.3. Lengthening corporal manoeuvres
Penile length restoration with the use of the sliding technique and concomitant PPI was first described in a small series of three patients in 2012, and further supported by a larger series of 28-patient in a multi-centre study in 2015 [1215,1219]. Although this technique is only used in cases of end-stage PD with severe shortening of the shaft, 95% of men were satisfied with the increase in length, with an average penile lengthening of 3.2cm (range, 2.5-4cm). The MoST and MuST are further modifications of the original sliding technique [1216,1217]. In a series by Egydio et al., 143 patients with penile shortening and narrowing due to PD amongst other aetiologies underwent MoST or MuST procedures. The mean (range) penile length gain was 3.1 (2-7) cm at a median (range) follow-up of 9.7 (6-18) months [1216].
9.3.2.c.4. Total phallic reconstruction
Radial forearm free flap is the most used reconstructive approach for TPR. In a single-centre study, Falcone et al., reported their experience of ten patients who underwent TPR using radial forearm free flap after traumatic penile loss [1355]. In six individuals, the urethral stump was sufficient for primary anastomosis and neourethra formation. The remaining patients had total penile avulsion and were voiding via a perineal urethrostomy. Consequently, a two-stage urethroplasty was necessary. Two patients developed an acute arterial thrombosis of the microsurgical anastomosis, which was successfully treated with emergency exploration. One patient had a neourethral stricture and fistula that required revision. All patients who underwent complete urethral repair were able to void and ejaculate through the phallus. After a median follow-up of 51 months, all patients were satisfied with the acquired size, cosmesis and sensation. Six patients received a PPI and were able to engage in penetrative intercourses. Three patients had revision surgery (two due to infection and one due to mechanical failure) [1355].
9.3.2.c.5. Summary of evidence and recommendations for surgical treatment of acquired penile shortness
| Summary of evidence | LE |
| Penile prosthesis implantation is not effective in increasing penile length. | 3 |
| The evidence for the use of penile disassembly manoeuvres and the sliding technique is limited. | 3 |
| Total phallic reconstruction yields satisfactory outcomes despite the high incidence of postoperative complications. | 3 |
| Recommendations | Strength rating |
| Do not recommend penile prosthesis implantation, penile disassembly or sliding technique to patients seeking penile lengthening options. | Strong |
| Use total phallic reconstruction to restore genital anatomy in genetic males with penile inadequacy due to traumatic loss. | Weak |
9.3.2.d. Penile girth enhancement
9.3.2.d.1. Penile girth enhancement history
Mean flaccid penis circumference is 9.31cm (± 0.90cm), and the erect penile circumference is 11.66 ± 1.10cm [1242]. Unlike penile lengthening, there are no precise definitions or indications for penile girth enlargement in the literature or existing international guidelines [1356]. Men have increasingly approached urologists for penile girth enhancement to increase their self-confidence, to be cosmetically satisfied, or to satisfy their partners [1357]. There are reports on penile girth enhancement techniques [1357,1358]. Although these surgical techniques are more frequently requested, the level of evidence supporting their use in clinical practice is low, and this is further compounded by the ethical considerations of surgery in this vulnerable patient group.
9.3.2.d.2. Injection therapy
Injectable filling materials can be classified according to their different properties. They can be autologous, biological or synthetic in nature. The fat injection material is obtained from the patient’s own tissue (autologous), usually by liposuction (see the following surgical therapy section). Biological fillers can be of human and animal (collagen) or bacterial (HA) origin. Poly-l-lactic acid (PLA), hydroxyethyl methacrylate, polyalkylimide hydrogel (PAAG), polymethylmethacrylate (PMMA), calcium hydroxyapatite (CHA), silicon and paraffin constitute filler materials of synthetic origin (Table 9.5) [1359].
Table 9.5: Origin of injectable filling materials
| Autologous | Autologous fat tissue |
| Biological | Hyaluronic acid |
| Synthetic | Poly-l-lactic acid, hydroxyethyl methacrylate, polyalkylamide hydrogel, polymethylmethacrylate, calcium hydroxyapatite, silicon, paraffin |
9.3.2.d.2.a. Soft tissue fillers (HA and PMMA)
Hyaluronic acid (HA)
Injection of HA gel is one of the most commonly used injectable fillers in the field of plastic surgery [1301,1360]. The application of HA for penile girth enhancement has gained increasing popularity due to its biocompatibility and infrequent mild temporary side effects.. Hyaluronic acid has been used for patients for penile girth enhancement. Studies have reported that an increase of 1.4 to 3.78cm in penile girth is achieved with HA injection (Table S9.6 online supplementary evidence Appendix 5). Patient satisfaction is high (78-100%) and no severe side effects have been reported [765,1361-1364].
Polymethylmethacrylate (PMMA)
Polymethylmethacrylate microspheres have been injected as a wrinkle filler. An average increase in penile circumference of 3.5cm was reported in two studies using PMMA for penile girth enhancement [1365,1366]. The authors reported that postoperative swelling and inflammatory reaction resolved within a few days and no pattern of PMMA microspheres migration to neighbouring regions was seen.
Poly-l-lactic acid (PLA)
Poly-l-lactic acid is another widely used soft tissue filler. Poly-l-lactic acid has enhanced effects by stimulating fibroblast proliferation and increasing collagen deposition in tissue. An average increase of 1.2 to 2.4 cm has been reported in the penile girth with PLA injection. No complications other than temporary local pain and swelling were reported in the treated patients [1361,1367].
9.3.2.d.2.b. Other Fillers (silicone, paraffin)
Foreign body injections are still frequently practiced in many countries (especially in East Asia and Eastern Europe), either by the patients themselves or by healthcare workers, using various substances such as paraffin, silicone or petroleum jelly (Vaseline), to increase the circumference of the penis [1368]. This induces a chronic granulomatous inflammatory foreign-body reaction [1368,1369] and leads to a pathological condition called sclerosing lipogranuloma of the penis, also referred as paraffinoma or siliconoma according to the substance used [1368]. The resultant inflammatory process ranges from oedema and infection to Fournier’s gangrene. Penile reconstructive surgeries may be required when siliconoma and paraffinoma require excision [1368-1374].
9.3.2.d.3. Surgical therapy
9.3.2.d.3.a. Autologous fat injection
Autologous fat injection is a surgical technique based upon thinning the lower abdomen with liposuction and injecting the harvested fat tissue into the penile shaft [1375-1378]. In retrospective studies, an average increase of 2 to 3.5cm in penile circumference was reported in patients who underwent autologous fat injection.
No statistically significant decrease was observed in IIEF scores and no serious adverse events, such as penile abscess or deformity requiring reoperation occurred. Postoperative satisfaction survey showed that more than 75% of patients were satisfied (Table S9.7 of the online supplementary evidence) [1343,1375,1376,1379].
9.3.2.d.3.b. Grafting procedures (albugineal and peri-cavernosal)
Until more rigorous multi-institutional studies report on complications and validated outcomes, penile girth enhancement procedures using grafts should be considered experimental (Table S9.8 of the online supplementary evidence and in Appendix 5).
In a study of 69 patients using the porcine dermal acellular matrix graft (InteXen; American Medical Systems, Minnetonka, MN, USA) a 3.2cm increase in flaccid state and 2.4cm in erect state was reported at one year following surgery. The procedure was performed with an infrapubic incision and 68 of 69 patients reported significant satisfaction using the APPSSI. Graft fibrosis has been observed in up to 13% of patients, and a mean reduction in penile length of 0.5cm was reported in patients with fibrosis [1380].
Techniques using venous grafts for penile girth enhancement have also been described [1381]. Initial results are encouraging, but better designed RCTs are needed.
Dermal fat grafts are free-only grafts composed of deepithelialized dermis and subcutaneous fat. An area of approximately 10 x 5cm is required for graft harvesting. With the dermal fat graft technique, an increase in penile girth of 1.67 to 2.3cm has been reported. Penile oedema up to 27%, painful erection up to 27%, and curvature due to graft fibrosis up to 9%, have been reported. Side effects such as penile hypoesthesia, skin necrosis and infection were not reported [1314,1382,1383].
9.3.2.d.3.c. Biodegradable scaffolds
This is a technique based on using fibroblasts (harvested from patients’ own scrotum skin and dartos tissue) in tissue cultures and seeding them in microporous biodegradable poly-lacti-co-glycolic acid scaffolds and implanting these scaffolds between Dartos and Buck’s fascia. A limited number of studies have reported girth gain of up to 4.02cm with implantation of biodegradable scaffolds [1384-1386] (see Table S9.9 of the online supplementary evidence or Appendix 5).
9.3.2.d.3.d. Subcutaneous penile implant (Penuma®)
A silicone penile implant called “Penuma®” (International Medical Devices, Beverly Hills, CA, USA) has been approved and has shown promising results for penile girth enhancement. Penuma® is a soft silicone subcutaneous implant placed on three-quarters of the penile shaft and fixed to the glans using a polyester mesh [1387]. Studies have reported an average increase in penile circumference of 2 to 5cm with Penuma® insertion. According to published data, complication rates (usually mild and transient, occur in < 5%) and the removal rate (1%) of the implant is reported as relatively low [1387,1388].
9.3.2.d.4. Summary of evidence and recommendations for penile girth enhancement
| Summary of evidence | LE |
| Various surgical approaches with specific outcomes and complications have been considered to address penile girth enhancement, with limited benefit. | 3 |
| Hyaluronic acid, PLA, hydroxyethyl methacrylate, polyalkylamide hydrogel (PAAG), PMMA, or CHA are used as injectable materials for penile girth enhancement. | 3 |
| Patient satisfaction with soft tissue fillers (especially HA, PMMA and PLA) is high (> 78%). | 3 |
| No complications other than temporary local pain and swelling were reported in patients treated with soft tissue fillers. | 3 |
| Using silicone, paraffin and petroleum jelly (Vaseline) in penile girth enhancement can lead to complications ranging from oedema to infection and Fournier’s gangrene. | 3 |
| Not enough long-term data are available on autologous fat injection for penile girth enhancement. | 4 |
| Not enough long-term data are available on grafting procedures (dermal acellular matrix graft, venous grafts or dermal fat grafts). | 4 |
| Grafting procedures are associated with high complication rates and low rates of patient satisfaction. | 3 |
| Not enough long-term data are available on biodegradable scaffolds and subcutaneous penile implant (Penuma®). | 4 |
| Recommendations | Strength rating |
| Counsel patients extensively regarding the risks and benefits of penile girth enhancement techniques. | Strong |
| Do not use silicone, paraffin and petroleum jelly (Vaseline) to address penile girth enhancement. | Strong |
| Use hyaluronic acid (HA), soft tissue fillers and autologous fat injection to address penile girth enhancement. | Weak |
| Do not use HA, soft tissue fillers and autologous fat injection to address penile girth enhancement in males with penile dysmorphic disorder. | Strong |
| Do not use grafts in penile girth enhancement, as they are considered experimental. | Strong |
| Do not use biodegradable scaffolds and subcutaneous penile implant (Penuma®) to address penile girth enhancement, as they are considered experimental. | Strong |
Figure 9.1: Management of short penile size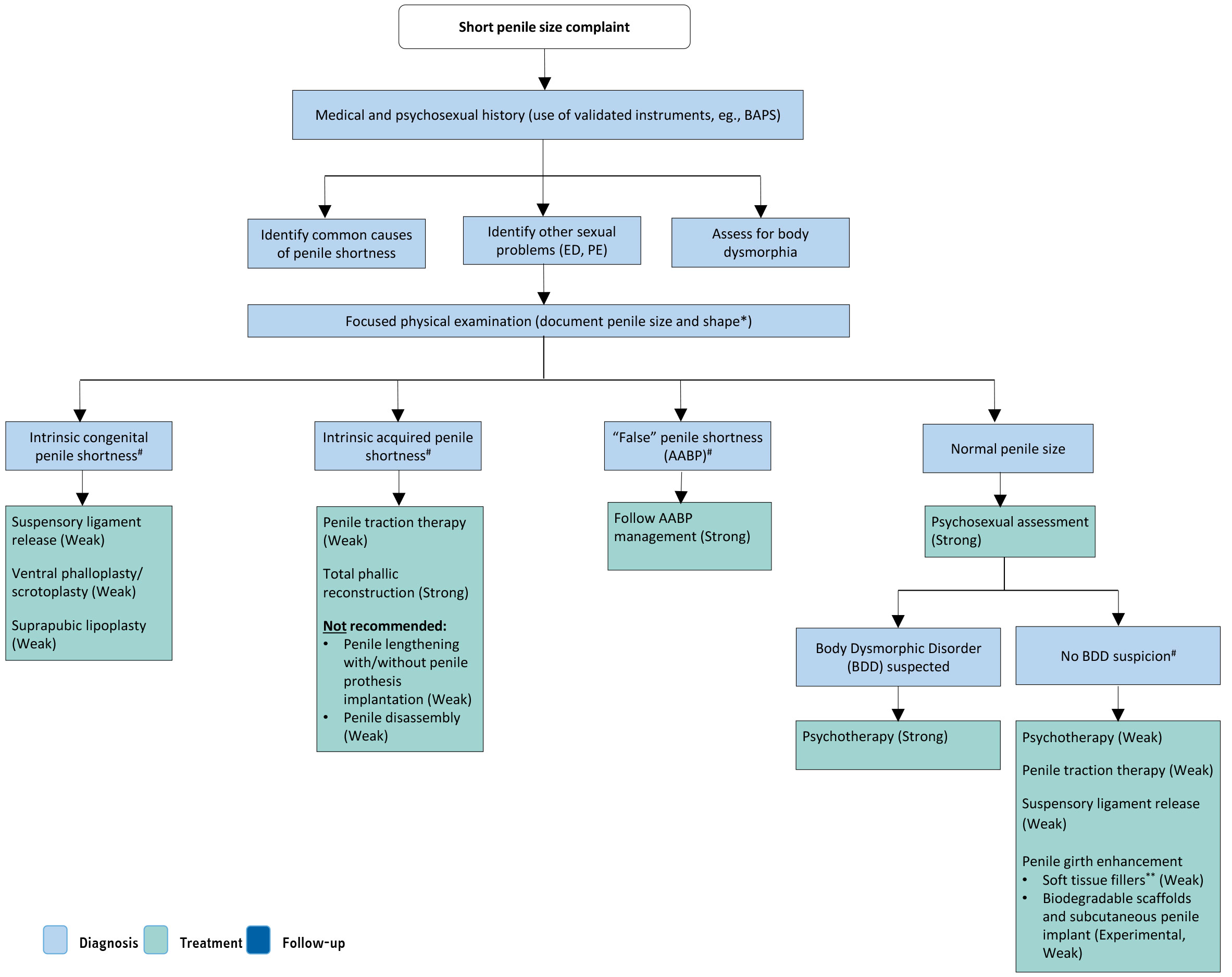 * Penile length should be measured stretched both from penopubic STT and from the pubic BTT.
* Penile length should be measured stretched both from penopubic STT and from the pubic BTT.
# There is lack of evidence to recommend one treatment over another.
** HA, PLA, hydroxyethyl methacrylate, PMMA, PAAG and CHA are considered as injectable materials for penile girth enhancement. Although the level of evidence is low, there is more evidence for HA, PLA and PMMA. Do not use silicone, paraffin or Vaseline (Strong evidence against).Strength of recommendations is depicted between brackets where appropriate.
AABP = adult acquired buried penis; BAPS = Beliefs about Penis Size Scale; BDD = body dysmorphic disorder; BTT = bone-to-glans tip; CHA = calcium hydroxyapatite; ED = erectile dysfunction; HA = hyaluronic acid; PAAG = polyalkylamide hydrogel; PD = Peyronie’s disease; PLA = poly-l-lactic acid; PMMA = polymethylmethacrylate; STT = skin junction-to-glans tip.
9.3.2.e. Functional outcomes: sexual function, sensitivity, impact on quality of life and emotional adjustment
Cosmetic treatments, including surgery, help to restore self-esteem and to reduce anxiety, social phobia, and depressive mood states regarding body concerns, increasing individuals’ well-being and QoL [1229,1230]. Therefore, we can expect males with genuine short penis to use available resources to adjust the length or girth of their penis to improve their sense of identity and fit cultural standards regarding penile size and function. Currently, the results of penile augmentation techniques appear mixed. The use of fillers resulted in improved genital self-image and self-esteem, as well as lower PDD symptoms, but no effects were found regarding self-confidence or sexual relationship satisfaction [1321]. Likewise, penile lengthening or girth enhancement surgery seem to result in poor satisfaction, EF and sensitivity in males with normal penis size [1240]. Despite those negative outcomes, cases of increased satisfaction have been registered [1389]. Male genital self-image has been related to IIEF domains: sexual desire, orgasmic and EF, intercourse, and overall satisfaction [1311]. Similarly, perceived penis size seems to predict EF more than objective size [1236]. In addition, reduced penetrative and receptive oral sex are associated with men’s dissatisfaction regarding their penis [1390]. For these reasons, more efforts should be made to clarify the impact of penile augmentation treatments on men’s and partners’ well-being and QoL. Males with BDD have shown reduced erectile and orgasmic function, as well as lower intercourse satisfaction compared with controls, whereas males with SPA demonstrated reduced satisfaction. Sexual desire seemed untouched in BDD and SPA cases [1321,1391].
9.3.2.f. Final remarks
The complaint of 'short penis' is variable in presentation and aetiology. Some patients demonstrate anatomical and pathological conditions while others do not. A vast array of treatments for different aetiologies of 'short penis,' both surgical and non-surgical, have been reviewed. If psychopathological symptoms are detected, the patient must be referred for further medical diagnosis. Treatment for short-penis syndrome requires a multidisciplinary approach, including medical and ethical considerations, and many reported outcomes are based on a paucity of evidence.