
13. DAYTIME LOWER URINARY TRACT CONDITIONS
13.1. Terminology, classification, epidemiology and pathophysiology
Normal storage and emptying of the bladder at a socially accepted place and time is mostly achieved by age three to four. Children with LUT conditions would present with failure to achieve continence (being still wet after the age of four), urgency, weak stream, hesitancy, frequency and accompanied UTIs. Isolated night-time wetting without any daytime symptoms is known as ‘enuresis’ and considered as a different entity [633] (See Chapter 14).
Urinary incontinence in children may be caused by congenital anatomical or neurologic abnormalities such as ectopic ureter, bladder exstrophy or myelomeningocele (MMC). In many children, however, there is no such obvious cause for the incontinence, and they are referred as having functional bladder problems. The most recent International Children’s Continence Society (ICCS) document suggests using the term daytime lower urinary tract (LUT) conditions to group together all functional bladder problems in children [633]. As different studies have used varying definitions and criteria, it is difficult to give reliable percentages regarding the prevalence, ranging from 2–25%. In general, an age dependent trend is seen with decreasing prevalence with increasing age [634-638].
Various factors have been associated with an increased incidence of daytime LUT conditions. Risk factors for developing overactive bladder (OAB) are obesity, a history of UTIs, nocturnal enuresis, a family history of LUT conditions, age of potty training, and bowel symptoms [639,640]. Daytime LUT conditions are more frequently encountered in children if the father was also affected during childhood [641]. The coexistence of constipation, LUT conditions and recurrent UTI is well described [642]. There is no evidence to conclude if bladder problems or bowel problems are the leading cause. The prevalence of constipation in older children varies from 5–27%, approximately 90% is functional constipation without an organic cause. In children with functional constipation the prevalence of bladder symptoms has been shown to be as high as 64% [643,644].
A link between daytime LUT conditions and neuropsychiatric developmental disorders such as ADHD (attention deficit/ hyperactivity disorder) has also been shown. In a meta-analysis there was a strong association between ADHD and LUTD in children, with an odds ratio for ADHD amongst children with LUTD of 2.99 (95% CI: 1.13–7.88, p < 0.001) [645]. Patients with neuropsychiatric developmental disorders usually are more likely to have more severe BBD at presentation, a lower QoL, and higher treatment resistance compared to those without a neuropsychiatric developmental disorder [646]. Furthermore, it is important to understand that in children with neuropsychiatric developmental disorders the pharmacological treatments influence concomitant bladder dysfunction, in both positive and negative ways [647].
Disturbances of the filling phase, the voiding phase or a combination of both in varying severity can be seen in children. The conditions are divided into either OAB or dysfunctional voiding. They can, of course, coincide and one may even be causative of the other. A specific type of incontinence in children is giggle incontinence. This is a sudden and involuntary episode of urinary incontinence provoked by laughter [648]. Dysfunctional bowel emptying may also be part of the clinical problems and BBD is the term used to cover concomitant bladder and bowel disturbances [633].
13.1.1. Filling-phase (storage) dysfunctions
In filling-phase dysfunctions, the detrusor can be overactive, as in OAB. Overactivity of the bladder is the most common problem, seen mostly around five to seven years of age. This may lead to disturbances characterised by urgency, frequency and at times urgency incontinence. Some children habitually postpone micturition leading to voiding postponement. Therefore, holding manoeuvres such as leg crossing and squatting can often be seen in this group. Recurrent UTIs are common and high-pressure state of the bladder can be a cause for VUR.
13.1.2. Voiding-phase (emptying) dysfunctions
In voiding-phase dysfunctions, the detrusor can be underactive, as in underactive bladder. In children with an underactive detrusor, voiding occurs with reduced or minimal detrusor contractions with post-void residuals. Urinary tract infections, straining to void, constipation and incontinence is common. Incontinence often occurs when the bladder is over-distended in the form of overflow incontinence.
During the voiding-phase incomplete relaxation or tightening of the sphincteric mechanism and pelvic floor muscles results in staccato voiding pattern (continuous urine flow with periodic reductions in flow rate precipitated by bursts of pelvic floor activity) or an interrupted voiding pattern (unsustained detrusor contractions resulting in infrequent and incomplete voiding, with micturition in fractions). The general term for this condition is dysfunctional voiding and is associated with elevated bladder pressure and PVR. Symptoms will vary depending on the severity of dyscoordination between bladder and the sphincter. Staccato voiding is seen in less severe forms and interrupted voiding and straining is seen in more severe forms.
In dysfunctional voiding, high voiding pressures generated by bladder working against a functional obstruction caused by non-relaxing sphincter may induce not only UTIs but also VUR. It has been shown that LUTD is more significant for the occurrence of UTI than VUR itself [649]. In the majority of children with dysfunctional voiding the recurrent infections disappear following successful treatment, which confirms the hypothesis that dysfunctional voiding is the main factor responsible for the infections. Spontaneous resolution of VUR may also be seen after successful treatment of dysfunctional voiding.
13.2. Diagnostic evaluation
13.2.1. History and physical examination
When evaluating a child with LUT conditions, a comprehensive, structured medical history should be performed. Furthermore, a voiding diary should be taken for a minimum of two days, which includes micturition frequency, voided volumes, night-time urine output, number and timing of incontinence episodes and fluid intake. History taking should also include assessment of bowel function. For evaluation of bowel function in children, the Bristol Stool Scale is an easy-to-use tool [650,651]. Several instruments and questionnaires are available to assess LUT conditions and have shown adequate results for clinical and research use [652].
During clinical examination, genital inspection should be performed to rule out abnormalities of the genitalia or meatus, and the lumbosacral spine and lower extremities should be investigated to evaluate a possible neurological cause.
13.2.2. Ultrasound and urinalysis
Using US to measure rectal diameter predicts the presence of constipation and correlates well with symptom improvement in children with BBD [653,654]. Urinalysis and urinary culture are essential to evaluate for a UTI, since transient voiding symptoms are common in the presence of UTI. In patients with recurrent UTIs and dysfunctional voiding, the upper urinary tract needs to be evaluated as well, using US and/or voiding cystography.
13.2.3. Urodynamics
Uroflowmetry with post-voiding residual (PVR) evaluates the voiding and emptying ability of the bladder. This can be combined with pelvic floor electromyography to demonstrate overactivity of the pelvic floor muscles during voiding. A flow rate which reaches its maximum quickly and levels off (‘tower shape’) may be indicative of OAB whereas interrupted or staccato voiding patterns may be seen in dysfunctional voiding. Plateau uroflowmetry patterns are usually seen in anatomic obstruction of flow. A single uroflowmetry test may not always be representative of the clinical situation and multiple uroflowmetry tests, when all give a similar result, are more reliable. Uroflowmetry examination should be done when there is desire to empty the bladder and the voided volume should at least be 50% of the age-expected capacity ([age in years] + 1) x 30 mL for the children. While testing the child in a clinical environment, the impact of stress and mood changes on bladder function should also be taken into account [633,655]. Some caution is warranted while interpreting uroflowmetry patterns, since inter-rater agreement for analysing uroflow curve pattern based on the ICCS criteria are variable [656].
Sometimes, there are (minor) underlying urological or neurological problems, which can only be diagnosed using (video)-urodynamic (VUD) studies or neurological evaluation. Video-urodynamics can be considered as well for patients with therapy-resistant dysfunctional voiding who are not responding to treatment and who are being considered for invasive treatment [657-659]. If neurological disease is suspected, MRI of the lumbosacral spine and medulla can help to exclude spinal dysraphisms such as tethered cord. Video-urodynamics may also be used as an initial investigational tool in patients with suspicion of reflux. In this case reflux may be observed along with bladder dynamics. Given the invasive nature of VUD, consider adequate distraction techniques and proper education of what to expect. Video-urodynamics in children can be performed with transurethral and suprapubic catheters, depending on the clinical question, and can be performed on the same day, also after placement of the suprapubic catheter [660]. However, performing VUD under general anaesthesia is not advisable [661].
13.3. Management
The treatment of daytime LUT conditions involves a multimodal approach, which is summarised in Figure 7.
13.3.1. Urotherapy and specific add-on interventions
Behavioural modification, mostly referred to as urotherapy, is a term which covers all non-pharmacological and non-surgical treatment modalities. It includes standardisation of fluid intake, bowel management; timed voiding and basic relaxed voiding education. The child and family are educated about normal bladder function and responses to urgency. Voiding regimens are instituted and UTIs and any constipation are treated. Treatment is aimed at optimising bladder emptying and inducing full relaxation of the urinary sphincter or pelvic floor prior to and during voiding [662].
Strategies to achieve these goals include [662]:
- Information and demystification, which includes explanation about normal LUT function and how a particular child deviates from normal function.
- Instructions about what to do about the problem:
- Regular voiding habits, sound voiding posture, pelvic floor awareness and training to relax pelvic floor and avoiding holding manoeuvres.
- Lifestyle advice, regarding fluid intake, prevention of constipation, etc.
- Registration of symptoms and voiding habits using bladder diaries or frequency-volume charts.
- Support and encouragement via regular follow-up by the caregiver.
Recurrent UTIs and constipation should also be treated and prevented during the treatment period. In case of combined BBD it is advised to treat the bowel dysfunction first as LUT conditions may disappear after successful management of bowel dysfunction [663].
Treatment efficacy can be evaluated by improvement in bladder emptying and resolution of associated symptoms. A high success rate has been described for urotherapy programmes, independent of the components of the programme. A Cochrane analysis found little evidence that can help to make evidence-based treatment decisions [664]. However, the evidence level is low as most studies of urotherapy programmes are retrospective and non-controlled.
In order to improve the outcomes of urotherapy for therapy-refractory children, specific interventions can be added, including biofeedback, physiotherapy (e.g. pelvic floor exercises), alarm therapy and specialised training programs. Although good results with these treatment modalities have been reported, the level of evidence remains low, since only a few RCTs were published [665,666].
In a meta-analysis, urotherapy including biofeedback training was effective for reducing UTIs and improving constipation. Furthermore, several urodynamic parameters improved compared to urotherapy alone [667]. The addition of pelvic floor muscle training to biofeedback improves outcomes in children with therapy-refractory DV with response rates of 59% [668]. Specialised training programs such as voiding school or bladder and bowel training programs show effective long lasting results in up to 46% of therapy-refractory children [669,670].
13.3.2. Medication
When considering medical treatment for OAB, there are several options in the paediatric population. Anticholinergic agents are still the mainstay of medical treatment, and oxybutynin is most commonly used [671]. However, the response to anticholinergics varies and many children experience side effects such as dry mouth and constipation. Although there have been reports about the use of tolterodine, fesoterodine, trospium, propiverine, and solifenacin in children, most of them are off-label depending on age and national regulations. Given the paucity of good-quality data on safety and tolerability, these medications should be used cautiously in children with close monitoring for potential side effects [672-675]. Despite the low level of evidence for the use of anticholinergics, their use is recommended because of the large number of studies reporting a positive effect on OAB symptoms. Although α-blocking agents are used occasionally, an RCT showed no benefit [676].
In recent years, the evidence supporting the effectiveness and safety of Mirabegron has been confirmed in several studies for children with OAB; however, it is still off-label for this indication in children. These results have been summarised in a systematic review by Kim et al. [677]. Both for monotherapy as well as add-on therapy improvement in continence has been reported [678,679]. Furthermore, starting mirabegron after symptom recurrence after previous Botulinum toxin A (BoNT-A)-injections resulted in a lower need for additional BoNT-A-injections. In a prospective RCT including patients with newly diagnosed OAB, patients were randomised for either mirabegron 50mg, solifenacin 5mg or placebo [680]. After the three months study period, the overall success rate was significantly higher in both the mirabegron and solifenacin group when compared to placebo. Furthermore, patients with mirabegron had significantly fewer side effects from treatment. These findings could support the use of mirabegron in an earlier stage for treatment of OAB. In a systematic review, including three studies with patients with OAB, it is shown that the administration of mirabegron to the paediatric population is cardiovascular safe with comparable efficacy to anticholinergic therapy [681]. Similar clinical results are reported for Vibegron, but need to be confirmed in larger studies [682,683].
13.3.3. Neuromodulation
Neuromodulation can be considered a second-line treatment after (standard) urotherapy and medical therapy have failed. Various types of neuromodulation are currently used to treat daytime LUT conditions with promising results; however, a direct comparison is difficult due to the different treatment regimens that are followed. Transcutaneous electrical nerve stimulation (TENS) has shown promising results in the treatment of OAB with improvement of symptoms and urodynamic outcomes, also when used as add-on treatment to anticholinergics [684-686]. Parasacral TENS is shown to be effective both as primary treatment or as an adjunct to standard urotherapy for daytime LUT conditions and faecal incontinence [687,688].
Posterior Tibial Nerve Stimulation (PTNS) is a minimally invasive treatment that demonstrated improved symptoms in therapy-refractory children as well as better QoL scores. This improvement has been shown to be long lasting in patients with OAB [689-691].
For therapy-refractory children sacral neuromodulation (SNM) has shown an improvement in symptoms of OAB; incontinence episodes, voiding frequency and QoL. This improvement is sustained in a certain group of children even after turning off the device. It is important to note that revision surgery may be necessary, especially in growing children [692].
13.3.4. Surgery
In patients with LUT dysfunction, cystoscopy should be performed when there is suspicion of lower urinary tract obstruction, and the subvesical obstruction should be treated. Although meatal correction was successful in correcting the direction of the urinary stream in 93% of girls with an anterior deflected urinary stream, only 29% of patients became continent afterwards [693]. Therefore, it should not be offered as a standard of care.
Intravesical BoNT-A can be considered as a second-line treatment for OAB in children, especially for daytime incontinence, even though it is still used off-label [694]. Different dosages and type of toxin have been shown to be effective and safe. In patients with refractory non-neurogenic OAB symptoms, intravesical BoNT-A-injections are effective in enlarging bladder volume and reducing symptoms, particularly in the first six months after injection [695]. Furthermore, there are significant bladder capacity increases after second and third injections as well [696]. Intersphincteric BoNT-A shows promising results for children with therapy-refractory dysfunctional voiding, ideally in combination with urotherapy [697].
Figure 7: The treatment of daytime LUT conditions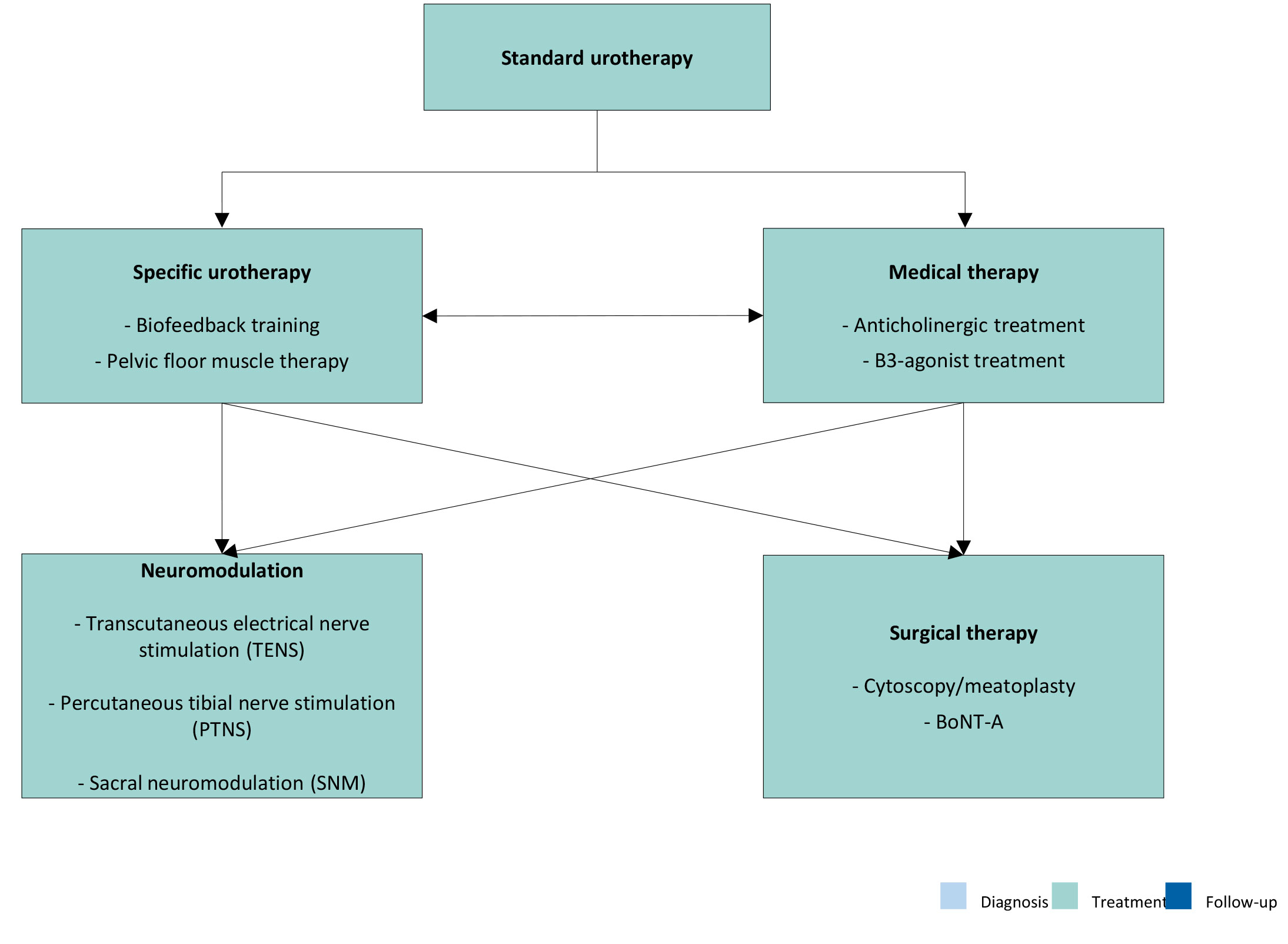
13.4. Quality of life
Symptoms of incontinence have a negative impact on the QoL of patients and their caregivers [698]. Successful treatment of LUT conditions significantly improves QoL for patients and their caregivers [699].
13.5. Follow-up
After an initial successful response to biofeedback, 20% of the patients relapse within two years [700]. Children treated for LUT conditions are more likely to have urinary tract symptoms later in life [701,702]. Furthermore, daytime wetting during adolescence showed a greater risk for mental health problems at the age of eighteen years [703]. Therefore, adequate transition into adult urology clinics is important when needed.
13.6. Summary of evidence and recommendations for the management of daytime lower urinary tract conditions
| Summary of evidence | LE |
| Daytime LUT conditions have a high prevalence. | 4 |
| Daytime LUT conditions are often seen in combination with constipation. | 2 |
| A correlation between daytime LUT conditions and neuropsychiatric developmental disorders has been demonstrated and more-severe symptoms are seen in children with neuropsychiatric developmental disorders. | 2 |
| Standard urotherapy includes standardisation of fluid intake, bowel management, timed voiding and basic relaxed voiding education. | 3 |
| Anticholinergic agents are the mainstay of medical treatment for daytime LUT conditions and Mirabegron has shown to be effective as monotherapy or add-on therapy. | 2 |
| Neuromodulation shows promising results as adjunctive treatment for urinary and faecal incontinence. Types of neuromodulation include transcutaneous electrical nerve stimulation, posterior tibial nerve stimulation and sacral neuromodulation. | 2 |
| Daytime LUT conditions negatively influences the QoL of patients and caregivers and successful treatment significantly improves QoL. | 2 |
| Children affected by daytime LUT conditions have a higher risk of urinary tract symptoms later in life. | 4 |
| Recommendations | Strength rating |
| Use two-day voiding diaries and/or structured questionnaires for objective evaluation of symptoms, voiding, drinking habits and response to treatment. | Strong |
| Use a stepwise approach, starting with the least invasive treatment in managing daytime lower urinary tract (LUT) conditions in children (see Figure 7). | Strong |
| Provide adequate bowel management as part of the treatment if bladder bowel dysfunction is present. | Strong |
| Re-evaluate in case of treatment failure. This may consist of (video) urodynamics, magnetic resonance imaging of lumbosacral spine and cystoscopy. | Weak |
| Arrange adequate transition into adult urological care for children with persistent daytime LUT conditions in adolescence. | Strong |