
19. URETEROCELE AND ECTOPIC URETER
19.1. Ureterocele
19.1.1. Epidemiology, aetiology and pathophysiology
Ureterocele is a cystic dilatation that develops in the intravesical part of the submucosal ureter but can extend extravesically. Ureterocele is four to seven times more frequent in female than male patients; the overall incidence in autopsies is around one in 4,000 children. Approximately 80% of ureteroceles are associated with the upper moiety ureter in duplicated systems: 20% are found in single systems and 10% of ureteroceles are bilateral [1132]. The aetiology remains unclear [1133-1135]. Ureteroceles can cause obstruction of the upper moiety, but the degree of obstruction and functional impairment is variable. Histological evaluation demonstrated that the changes represent a process of maldevelopment and may not result from infections or obstruction [1136]. The presence of an ureterocele in a duplicate system increases the risk for developing a febrile UTI [1137].
19.1.2. Classification systems
Orthotopic (intravesical) ureterocele
The intravesical or orthotopic ureterocele is completely located in the bladder and is mostly associated with a single kidney system. Orthotopic ureterocele is diagnosed more frequently in older children or adults. In the orthotopic form, there is often no or only mild obstruction and the function of the moiety is normal or slightly impaired. In duplex systems, vesicoureteral reflux can be observed in 50% on the ipsilateral side and 20% on the contralateral side. Reflux into the ureterocele is uncommon [1138].
Ectopic (extravesical) ureterocele
If any portion of the ureterocele extends into the bladder neck or urethra, this is referred to as an ectopic ureterocele, which is the most common form of ureterocele (> 80%). Ectopic ureterocele can be voluminous, dissociating the trigone and slipping into the urethra (caecoureterocele) and may prolapse through the urethral meatus . The ureterocele orifice is tight and located in the bladder itself or below the bladder neck. The ureter corresponding to the lower moiety is raised by the ureterocele and is frequently refluxing, but can also be compressed by the ureterocele, leading to an obstructive megaureter. A contralateral renal duplication is seen in 50% of cases. Occasionally, large ureteroceles are responsible for reflux or obstruction of the contralateral upper tract. In the ectopic ureterocele or caecoureterocele, the upper moiety is generally poorly functioning [1136].
19.1.3. Diagnostic evaluation
At present, antenatal US detects ureterocele in the majority of cases if associated with obstruction, and diagnosis is confirmed after birth by further investigations. Later in life, these anomalies can be complicated by clinical symptoms. There is a wide variation of symptoms in patients with ureterocele (from the asymptomatic patient to urosepsis, urinary retention and hydroureteronephrosis after birth).
Prenatal US easily reveals voluminous obstructive ureteroceles [1139]. In cases with a small upper moiety or a slightly obstructive ureterocele, prenatal diagnosis is difficult. Postnatally, the following clinical symptoms, besides incidental findings, can reveal the congenital anomaly at birth or later:
- At birth, a prolapsed and sometimes strangulated ureterocele may be observed in front of the urethral orifice in girls. In newborns, it might cause acute urinary retention.
- The early symptom of pyelonephritis in either sex may lead to the diagnosis.
- Later problems can include dysuria, recurrent cystitis, urgency, incontinence or stones.
In cases of prenatal diagnosis, at birth, US confirms the ureteral dilatation that ends at the upper moiety of a renal duplication. It also demonstrates the presence of a ureterocele in the bladder, with a dilated ureter behind the bladder. The diagnostic workup should assess the presence of bladder neck obstruction/insufficiency, vesicoureteral reflux, upper/lower moiety obstruction and upper/lower moiety function (Figure 12). VCUG is recommended for identifying ipsilateral or contralateral reflux, for assessing the bladder neck and the degree of intra-urethral prolapse of the ureterocele [1140]. However, in asymptomatic patients with an intravesical ureterocele without lower moiety dilatation, this step could possibly be omitted. Renal scintigraphy should be used to assess moiety function, which is best assessed with DMSA [1141]. Magnetic resonance urography may visualise the morphological status of the upper moiety and lower moieties and of the contralateral kidney and can detect renal scars [1142,1143]. Using functional MR urography, differential renal function can be assessed with low intra- and interobserver variability [1144]. Urethrocystoscopy may reveal the pathology in cases where it is difficult to make the differential diagnosis between ureterocele and ectopic megaureter.
19.1.4. Management
The management of an ureterocele in a duplex system is variable. When the diagnosis is made using US, prophylactic antibiotic treatment should be considered, particularly if the diameter of the distal ureter is > 7mm [613]. Furthermore, management can include active surveillance, endoscopic decompression and additional surgery through an upper approach (either partial nephroureterectomy, pyeloureterostomy or high ureteroureterostomy) or lower approach (low ureteroureterostomy, ureteral reimplantation or complete primary reconstruction) [1145-1150].
In a clinically asymptomatic child with a ureterocele, management is dependent on ultrasound findings, the presence of vesicoureteral reflux and moiety function (Figure 13). In case of a nonfunctioning upper moiety, without significant obstruction of the lower moiety and without bladder outlet obstruction, initial conservative management may be undertaken, including prophylactic antibiotic treatment. Continuation of conservative management is an option in asymptomatic patients without any bladder outlet obstruction, with minimal hydroureteronephrosis of the upper moiety or low-grade (< grade III) reflux, or ureteroceles with a dysplastic moiety [1150-1152]. However, in these patients, long-term follow-up is necessary [1153]. In 58% of patients, there is spontaneous resolution or improvement of lower moiety reflux [520]. In asymptomatic patients with a decreased upper/lower moiety function, surgical treatment should be considered for nephron preservation and/or prevention of UTI.
In the presence of urosepsis/pyonephrosis or obstruction at the bladder neck, immediate drainage is recommended. In severely sick children, nephrostomy drainage of the upper moiety can be considered as a first-line treatment. There are several techniques used for decompression, including cold-knife incision, electrosurgical incision and laser puncture. For orthotopic ureteroceles in particular, laser puncture shows superior results compared to electrosurgical incision with regard to secondary VUR and reoperation rate [1154]. Decompression of the dilated system facilitates later reconstructive surgery [1155,1156]. Moreover, two systematic reviews suggest that, after primary ureterocele incision, the rate of secondary VUR and the reoperation rate is higher in those with an ectopic ureterocele and in patients with a duplex system [1157,1158].
Additional surgery is required if primary decompression is not effective, if significant reflux is present, in case of obstruction of the ipsi- or contralateral ureters, or if there is bladder neck obstruction/insufficiency [1159]. As mentioned previously, this can be classified through an upper approach or lower approach [1149,1160-1162]. Several single-centre case series and non-randomised comparative studies have been published regarding these various approaches with good surgical and long-term outcomes [1163-1165]. The choice of a therapeutic modality depends on the following criteria: clinical status of the patient (e.g. urosepsis); patient age; function of the upper moiety; presence of reflux or obstruction of the ipsilateral or contralateral ureter; presence of bladder neck obstruction caused by ureterocele; intravesical or ectopic ureterocele; and caregivers’ and surgeon’s preferences [1150,1166]. A lower approach can be an option even in those with a poorly functioning or nonfunctioning upper moiety [1167]. The use of minimally invasive surgery, including laparoscopic, retroperitoneoscopic and robot-assisted techniques is increasing for both upper and lower approaches, with good surgical and long-term outcomes [1168-1170]. Several studies compared the minimally invasive high ureteroureterostomy versus low ureteroureterostomy, slightly favouring the lower approach regarding operative time and severity of complications, however, these studies were nonrandomised [1171-1173].
Despite favourable surgical outcomes, reconstructive surgery may not be necessary at all in some patients, as less aggressive surgical treatment and nonoperative management over time can achieve the same functional results [1174,1175]. Long-term follow-up after surgical reconstruction is recommended, since up to 27.4% of patients can develop LUTD after lower urinary tract reconstruction, after a mean follow-up of almost 10 years [1176].
Figure 12: Diagnostic and treatment pathway for symptomatic ureterocele VCUG = voiding cystourethrography; VUR = vesicoureteral reflux.
VCUG = voiding cystourethrography; VUR = vesicoureteral reflux.
Figure 13: Diagnostic pathway for asymptomatic ureterocele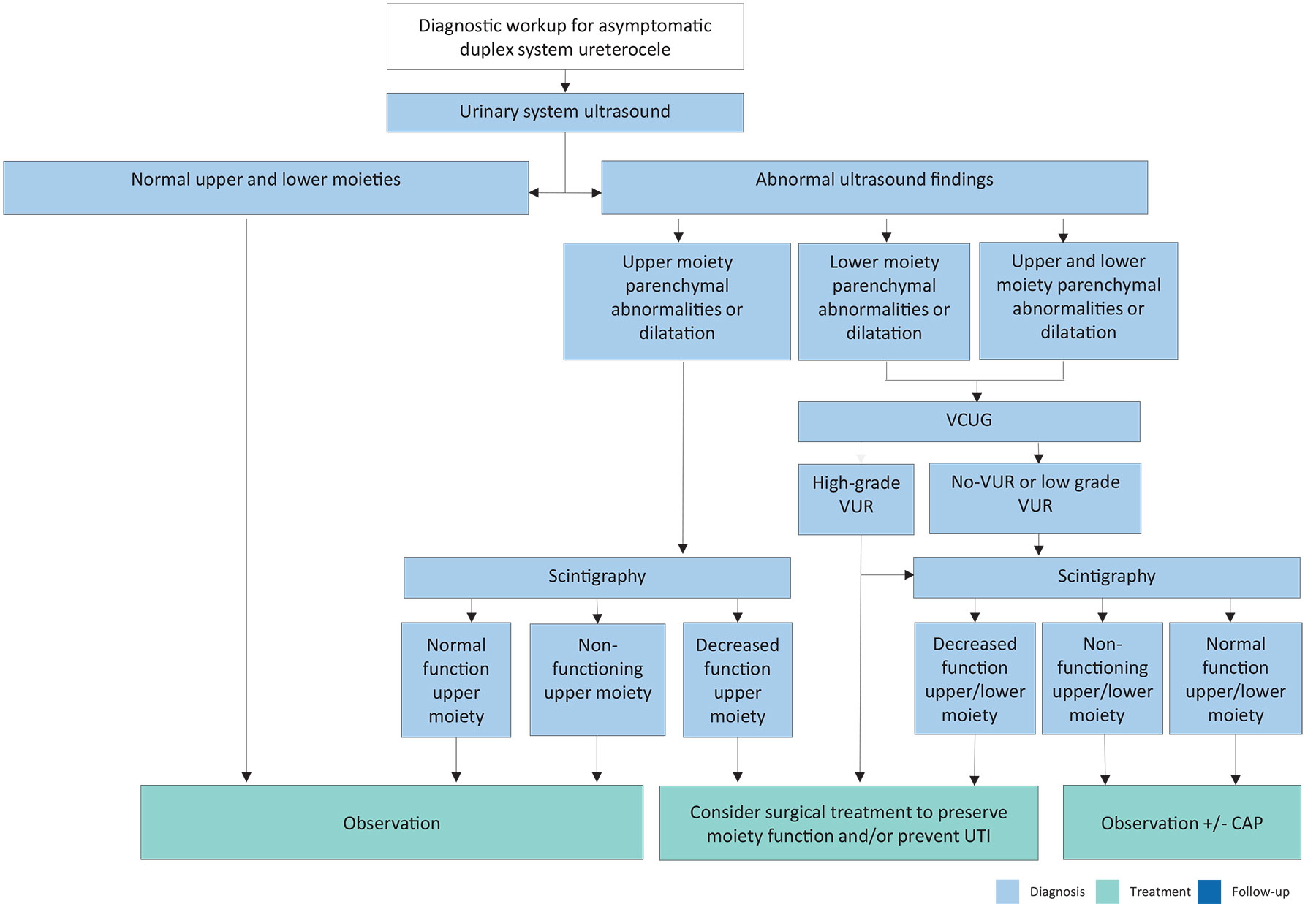
CAP = continuous antibiotic prophylaxis; UTI = urinary tract infection; VCUG = voiding cystourethrography; VUR = vesicoureteral reflux.
19.2. Ectopic ureter
19.2.1. Epidemiology, aetiology and pathophysiology
Ectopic ureter is less frequent than ureterocele (10 in 19,046 autopsies) and is more common in female patients as well (male to female ratio is 1:5). Some remain asymptomatic, therefore, the true incidence is difficult to determine [1177]. Eighty percent of ectopic ureters are associated with complete renal duplication. However, about 50% of ectopic ureters in male patients are associated with a single system [1178].
19.2.2. Classification
The term ‘ectopic ureter’ describes a ureter with the orifice located at the bladder neck, in the urethra or outside the urinary tract. The ureter can drain the upper moiety of a duplex or single system. There is a fundamental difference between the sexes. In boys, the ectopic orifice is never below the external sphincter.
In girls, the ureteral orifice may be located [1179]:
- in the urethra, from the bladder neck to the meatus (35%);
- in the vaginal vestibule (34%);
- in the vagina (25%); or
- in the uterus and fallopian tube (6%).
In boys, the ureteral orifice may be located [1179]:
- in the posterior urethra (47%);
- in the prostatic utricle (10%);
- in the seminal vesicles (33%); or
- in the vas deferens or ejaculatory ducts (10%).
19.2.3. Clinical presentation and diagnostic evaluation
Most of the ectopic ureters are diagnosed due to detection of an upper moiety ureterohydronephrosis in an asymptomatic child. In some cases, clinical symptoms can lead to diagnosis. In neonates, clinical manifestations may include pyuria and acute pyelonephritis. In young girls, persistent urinary incontinence despite normal voiding or significant vaginal discharge mimicking incontinence may be observed. In such cases, an ectopic orifice may be identified in the meatal or vaginal region [1180]. In preadolescent boys, a specific clinical presentation may be recurrent epididymitis, and the seminal vesicle may be palpable on physical examination. Ultrasound, radionuclide studies (DMSA/MAG-3), VCUG or MRI are diagnostic tools to assess function, to detect reflux and rule out ipsilateral compression of the lower moiety and urethral obstruction [1181]. In some cases, the large ectopic ureter presses against the bladder and can look like a pseudoureterocele [1182].
19.2.4. Management
In nonfunctioning moieties with recurrent infections or in girls with urinary incontinence due to continuous dribbling, surgery can be considered. Surgeries can be classified into an upper approach (partial nephroureterectomy, pyeloureterostomy or high ureteroureterostomy) or lower approach (low ureteroureterostomy, ureteral reimplantation or complete primary reconstruction). Reconstructive surgery should be considered, particularly in cases in which the upper moiety has function worth preserving. Similar to ureteroceles, all these procedures can be performed by means of an open, laparoscopic or robot-assisted approach with comparable results [1173,1183-1186]. In patients with bilateral single ectopic ureters (a very rare condition), an individual approach is necessary, depending on the sex and renal and bladder function of the patient. Usually, the bladder neck is insufficient in these patients [1187].
19.3. Summary of evidence and recommendations for the management of obstructive pathology of renal duplication: ureterocele and ectopic ureter
| Summary of evidence | LE |
| Ureterocele and ectopic ureter are usually associated with complete renal duplication, but they also occur in a single system. | 1 |
| Most infants are asymptomatic, while in older children, clinical symptoms will prompt assessment. The diagnosis is usually made by ultrasound. | 1 |
The choice of surgical treatment will depend on:
| 3 |
| Both for ureterocele and ectopic ureter, additional surgery can be performed either through an upper approach or a lower approach. | 1 |
| Recommendations | Strength rating |
| Start continuous antibiotic prophylaxis (CAP) in neonates with hydroureteronephrosis due to ureterocele or ectopic ureter. | Weak |
| Use imaging in patients with ureterocele/ectopic ureter to assess moiety function, reflux status and obstruction. | Strong |
| Offer drainage such as endoscopic decompression or nephrostomy for patients with infectious obstructive ureteroceles. | Strong |
| Choose additional treatment based on clinical status of the patient, age, moiety function, presence of reflux or obstruction of the ipsilateral or contralateral ureter, presence of bladder neck obstruction caused by ureterocele, intravesical or ectopic ureterocele, and caregivers’ and the surgeon’s preferences. | Weak |