
6. FERTILITY PRESERVATION IN CHILDREN AND ADOLESCENTS
The continuous increase in the incidence of paediatric cancers and post-treatment survivorship over the years, coupled with the further development of potentially gonadotoxic therapies, has contributed to the recognition and rapid endorsement of fertility-preservation counselling for prepubertal children and adolescents. Patients and caregivers should be informed not only about the impact of gonadotoxic treatments on future fertility, but also about fertility-preservation options and their risk-benefit ratio. There are also several nononcological congenital anomalies where fertility preservation can become an issue.
This chapter focuses on basic information on cryopreservation indications and options for paediatric urologists. For more detailed information, we refer to specific guidelines on this topic [212-214].
6.1. Ovarian tissue cryopreservation in prepubertal and adolescent girls
Infertility in the paediatric and adolescent population can result from direct gonadal damage from surgery, or gonadal toxicity as a result of chemotherapy or radiation [212]. Frequent indications requiring gonadotoxic therapy include solid tumours, leukaemia and benign indications, such as hemoglobinopathies [215]. First-line chemotherapy does not appear to affect the number of primordial follicles [216]. Rather, it seems to have a significant effect on the health, density and functionality of follicles [217], resulting in a reduction of 10-30% of ovarian reserve, depending on age and menarchal status [218]. The indication and options for fertility preservation should ideally be discussed in a paediatric multidisciplinary fertility preservation team and should consider the toxicity of the planned therapy, the age and menarchal status, as well as ethical and financial issues [219,220].
In paediatric and adolescent patients, ovarian tissue retrieval is performed by removal of an entire ovary (or partial ovariectomy) by laparoscopy [221], or in the setting of a laparotomy for surgery of the primary tumour [215,222]. It is advised to combine these interventions with other medically indicated procedures to minimise any additional anaesthetic risks and costs [223]. In postpubertal patients and in the setting of benign disease, oocyte retrieval following prior ovarian stimulation can be performed [224-227]. For patients undergoing brachytherapy of the pelvic region, the technique of temporary laparoscopic ovarian transposition has been described [228].
Ovarian tissue can be reimplanted orthotopically or heterotopically. For fertility purposes, orthotopic transplantation includes implanting ovarian tissue into the peritoneal cavity, the remaining contralateral ovary, the ovarian fossa or the broad peritoneal ligament [229]. Heterotopic transplantation includes transplantation of ovarian tissue into other locations, such as the subcutaneous abdominal wall, the rectus muscle and the forearm. This technique can be used for the recovery of natural endocrine function [229]. The utilisation rate of ovarian tissue for ovarian cortex autotransplantation in the paediatric population has been reported to be as low as 2.2-5% [226,230,231]. A large case series demonstrated that transplantation of prepubertal cryopreserved ovarian tissue resulted in induction of spontaneous puberty and pregnancies in a few reported cases. However, only a few cases with long-term outcomes are reported in the literature [232,233].
Figure 3: Ovarian tissue cryopreservation for girls and adolescents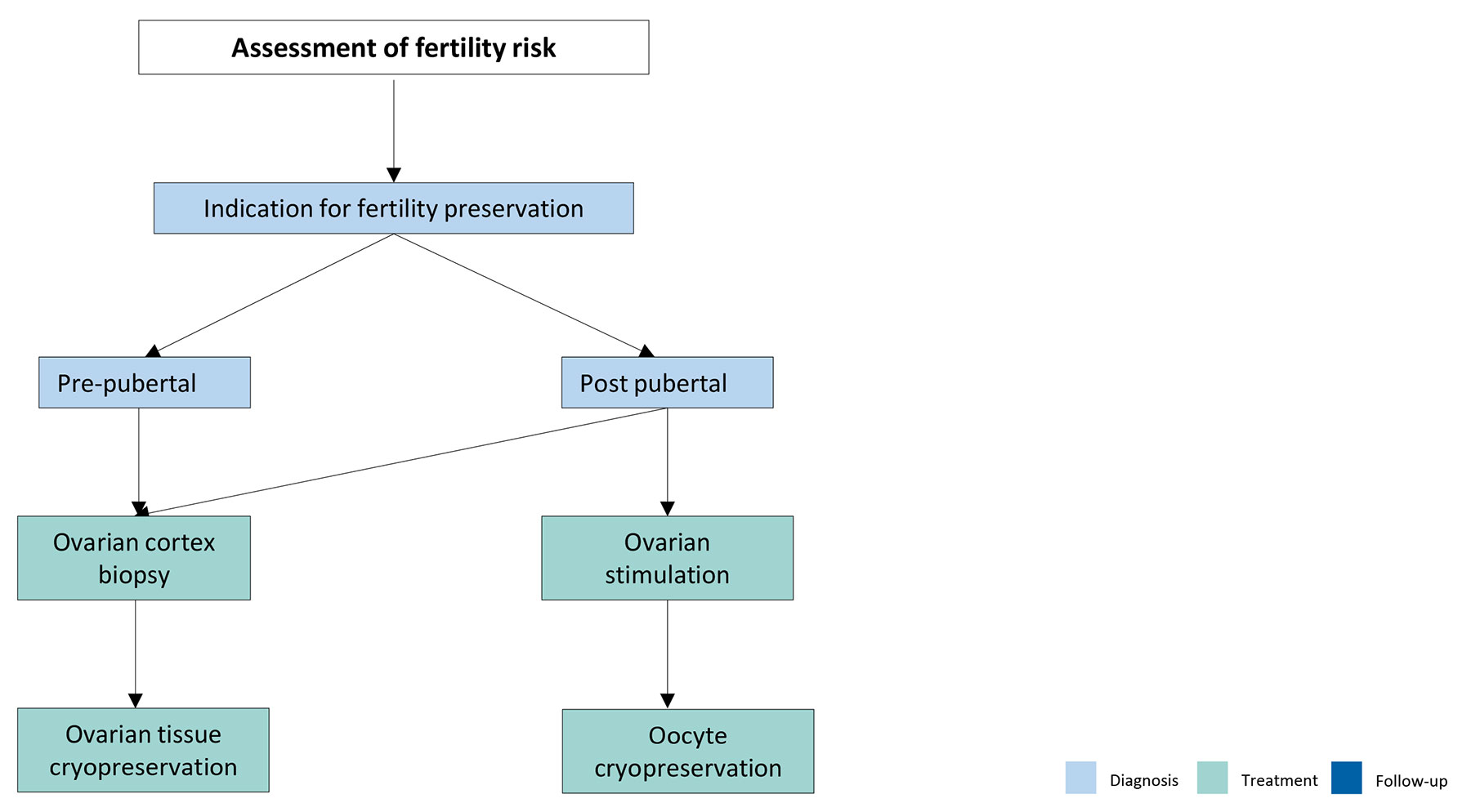 Adapted from Anderson et al., [227].
Adapted from Anderson et al., [227].
6.2. Cryopreservation in prepubertal and adolescent boys
The increase in the incidence of paediatric cancers and post-treatment survivors has also contributed to studies for fertility preservation in prepubertal boys. Gonadoprotective measures aiming at protecting the survival and function of immature germ cells in prepubertal testes, which are highly susceptible to irradiation and chemotherapy, should be the first aim [234]. Attenuation of externally scattered irradiation from fields close to the testes by gonadal shielding has been shown to be effective with respect to testicular growth in survivors [235,236]. In patients undergoing brachytherapy in the genital region, temporary testicular transposition has been described as a method for fertility preservation [237].
Sperm cryopreservation via masturbation or penile vibration should be the first option in nonazoospermic postpubertal boys. Techniques such as electroejaculation should only be discussed in very specific circumstances. Cryopreservation of immature testicular tissue, containing spermatogonial stem cells, as a fertility preservation option for this population is still experimental and should be carefully explained to caregivers and patients by a multidisciplinary team [234]. Testicular biopsy procedures do not seem to affect fertility potential, due to surgical complications or due to disruption of the blood-testicular barrier. However, further studies on this topic are needed [238].
Additional anaesthesia-related risks for testicular sampling should be avoided, if possible. The procedure can be combined with any other intervention requiring anaesthesia whenever possible [234].
For benign conditions such as Klinefelter Syndrome, with the potential risk of germ cell loss prior to puberty, bilateral undescended testes cryopreservation has been proposed but remains controversial and experimental [239-241].
Even though experimental advances have been achieved in non-human primates, many challenges remain to be addressed for prepubertal testes before clinical application.
6.3. Summary of evidence and recommendations fertility preservation in children and adolescents
| Summary of evidence |
| It is advised to combine any fertility preservation intervention with other medically indicated procedures to minimise additional anaesthetic risks and costs |
| Ovarian tissue cryopreservation can be used for fertility preservation in pre- and postpubertal girls. |
| Cryopreservation of immature testicular tissue, containing spermatogonial stem cells, as a fertility preservation option for this population is still experimental and should be well explained to caregivers and patients by a multidisciplinary team. |
| Recommendations | Strength rating |
| Inform patients and caregivers about the impact of gonadotoxic treatments on future fertility and about fertility preservation options and their risk-benefit balance. | Strong |
| Discuss the indications and options for fertility preservation in a paediatric multidisciplinary fertility preservation team and consider the toxicity of the planned therapy, the age and pubertal status as well ethical and financial issues. | Strong |