
27. TRANSITIONAL UROLOGY
27.1. Introduction
Transition in urology is defined as the process where an adolescent or young adult with a congenital or acquired urogenital anomaly transitions into adult services and begins to assume increasing responsibility for their own health care, thus becoming the primary decision-maker in their own care. The main goal of the transition process in urology is to preserve renal function, to optimise QoL by achieving and maintaining continence, to treat and manage issues related to sexuality and infertility, and to monitor for progression of the disease process or complications related to interventions [1544-1546].
27.2. Barriers in transition
The process of transition is different for each individual. It is dependent on a complex interplay of factors such as psychosocial development, the onset of puberty, and the persistence and severity of physical and congenital disabilities. The child, caregivers and urologists often have different views and expectations during transition, which can lead to inherent difficulties with noncompliance and failure of attendance. Adolescents expect to be more like their peers without disabilities and experience changes due to puberty, including the willingness to participate in health care agreements. Concurrently, paediatric urologists may opt to increase the number of visits to enable a smoother transition to the adult urologist, without any significant outstanding therapeutic issues. Caregivers may be reluctant to be discharged by the paediatric urologist with whom they had a long-standing relationship.
Finding an adult urologist with expertise in functional and reconstruction urology and with knowledge of both underlying congenital conditions and their optimal treatment can be challenging. The adult urologist must be focused on the overall care of the patient and be able to work in a multidisciplinary team to fill in the gaps of each individual discipline. Strong lines of communication between the relevant specialists are essential (e.g. nephrology, neurosurgery, gynaecology, rehabilitation doctors, orthopaedics) [1544-1547]. Specific key features have been identified that can pose difficulties in the transition process (Table 13).
Table 13: Key structural differences between paediatric and adult care that can pose difficulties in the transition process (adapted from Claeys et al., 2021 [1546])
| Feature | Paediatric care | Adult care |
| Patient management | Involvement of a large multidisciplinary team, often lead by a single provider (referrals within the team) | Smaller teams with subspecialty expertise (referrals to other specialties as needed) |
| Care approach | Family centred | Patient centred |
| Patient functioning | Limited independence | Expected independence |
| Clinic management | Time allotted for detailed discussion with intensive coordination | Usually, shorter appointment times and focused care coordination |
| Access to psychology | Good access | Often limited access |
| Follow-up | Regular active follow-up | More passive follow-up |
27.3. The transition process
The optimal age at which patients should transition into the care of adult providers has not been firmly established and may need to be individualised to the patient based on their unique situation. Overall, it is important to address transitional care from the age of 12 years, and by 16 years at the latest. A gradual introduction of the adult urologist into the health care team, several years before targeted time of transition, may facilitate the process of transition, as the child and the caregivers gain trust in the new provider [1548].
Early childhood transition planning should focus on developing long-term goals and expectations to promote optimal health and independence, lifelong care access, and financial planning. During the adolescent years, transition preparation should include developing a care plan, decision-making support, supporting self-management development, and addressing care coordination [1549].
Various models of a transition programs have been proposed. Although no single approach has been demonstrated as superior [1550]. The National Alliance to Advance Adolescent Health (https://www.gottransition.org/six-core-elements) has identified six core elements to support transitional care across specialties. For each element, several measures are proposed to allow for a successful transition to adult care. An ideal age for completion of each step is only a reference and may require adjustment based on the developmental stage of the child and legal definitions of the age of majority between country jurisdictions. Recommendations include, but are not limited to, the core elements shown in Figure 16.
Figure 16: Six core elements to support transition care across specialities
(adapted from https://www.gottransition.org/six-core-elements)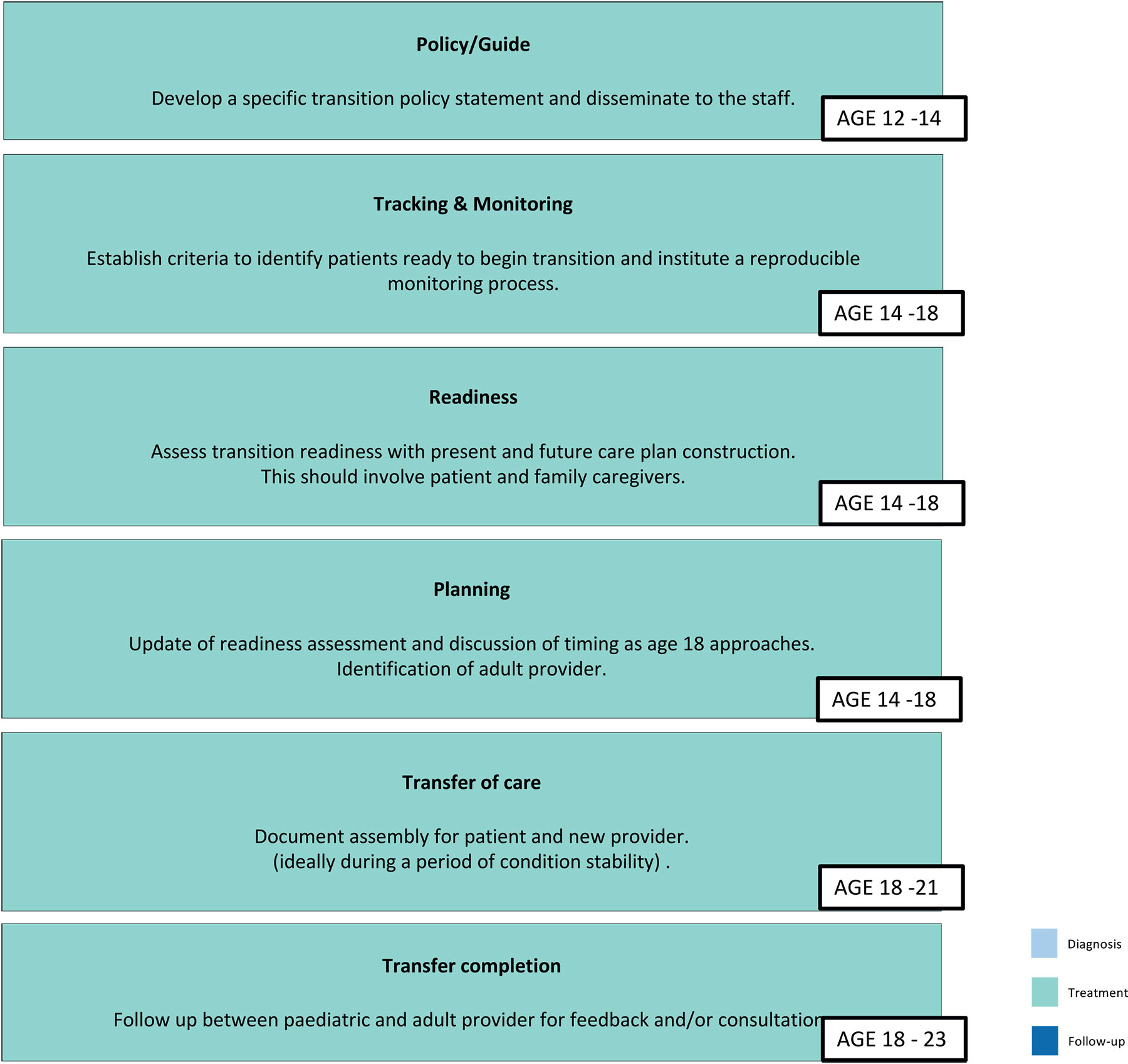
Assessment of readiness may be formalised using readiness assessment questionnaires completed by both the child and caregivers to provide insight into their ability to cope with the transfer process and, therefore, represents a way of determining when the right time is for them to meet adult-focussed health-care providers [1546]. Adaptation of the six core elements to urology transition enables the creation of a checklist of active and resolved issues, operative reports and elements for conditions surveillance (i.e. surveillance imaging studies, blood work) and an updated inventory of renal function, continence status, fertility/sexual function, bowel function and psychosocial status [1546,1551].
27.4. Specific genitourinary conditions
27.4.1. Neurogenic bladder
Renal and bladder function are closely linked in children, and those presenting at an adult urological clinic may have evidence of dysfunction or deterioration (without or without reconstruction), which increases the risk of renal damage. There is a wide range of aetiologies for bladder dysfunction in childhood, including bladder outlet obstruction, smooth muscle/sphincter dysfunction, abnormal bladder function, and spinal cord/brain abnormalities. These dysfunctions may also be acquired and include recurrent UTIs, stones, trauma, chemotherapy and/or radiotherapy, and iatrogenic interventions. The most common cause for neurogenic bladders in adolescent and transitional clinics is spinal dysraphism, of which myelomeningocoele is the most likely to cause bladder and bowel dysfunction [1552]. With advances in neonatal and paediatric care, 50-94% of infants born with spina bifida are now estimated to survive into adulthood [1553]. This means that adult urologists are increasingly encountering such patients and are tasked with managing the urological manifestations of this condition and/or its treatments, with healthcare providers requiring more than a basic knowledge of neurogenic bladder management. Specific urological issues at transition require surveillance and management of renal function, urinary incontinence, urinary tract infections, bowel function, sexual function, urolithiasis, and complications from urinary tract reconstruction [1554]. The risk of bladder cancer following augmentation in children appears to be very low. However, the data from a systematic review analysing this data was only able to include two studies with more than five-years follow-up. Therefore, long-term oncological outcomes remain uncertain [1555].
Several studies have demonstrated ongoing, underlying issues at presentation to adult urological clinics in this cohort. A joint study from Utah and Minnesota in the United States demonstrated that 77% patients were performing intermittent catheterisation, with 84.6% having an identified urological problem, the most common of which was bothersome urinary incontinence affecting 52% patients. Overall, 97% required an intervention [1556]. Another study demonstrated that following attendance at a transitional care clinic for spina bifida, 71% of adolescent/adult patients required changes in bladder management and 38% underwent a major surgery [1557]. In Canada, only a minority of paediatric urologists perceive that the transition process should begin at the age of eighteen or older. However, there is no defined ongoing urological care as a component of this process, suggesting the potential for substandard quality of care [1558]. This is in contrast to the 2023 Spina Bifida Association’s Transition to Adult Care Guidelines, which recommended that transition discussions should ideally begin at birth.
The process of transition is critical to a smooth transfer of care to adult services. A US study demonstrated that 40% patients had never wanted to transition, and that parents thought about this more than patients did. Only 34% patients had a transition plan, with the only significant predictor of transition being a history of urolithiasis [1559]. In a study examining sexual and reproductive health in adolescents with spina bifida, 95% patients stated that they had inadequate knowledge of these issues [1560]. Factors affecting transition readiness have included higher validated assessment scores (e.g. TRAQ; Transition Readiness Assessment Questionnaire), which is negatively associated with urinary incontinence, and positively associated with health literacy [1561,1562]. Despite this, a study from the United States of transitioned adults with spina bifida demonstrated on TRAQ scoring showed that they were still not fully ready to transition, with males affected more than females. This suggested that an increased attention to transition readiness and consideration of a longer transition process in this population may be necessary [1563,1564]. The frequency of clinic surveillance also appears important. Most adult spina bifida patients have symptomatic urological issues within a two-year follow-up interval, with 34% having significant issues within three years, which suggests a narrower interval frequency [1565]. The barriers to successful transition in spina bifida patients within TRAQ domains include ‘appointment keeping’ and ‘tracking health issues,’ as well as financial difficulties and the utilisation of community services. These indirect medical issues suggested that an increased awareness around transition readiness and the involvement of social work and specialist nursing were an integral part of the process [1566,1567].
Several studies have shown improved outcomes in spina bifida patients who have undergone formal transition compared to an ad hoc referral to adult services, with much of this data currently originating from North America. A study from Texas reported improved adherence to bowel regimens at the time of transfer to adult care, along with better planning for decision-making and transportation to clinic appointments [1568]. A separate study from Michigan found that females were more likely than males to attend clinics following transition to adult services, while individuals who did not transition had comparable outpatient visit patterns but higher rates of inpatient and emergency care utilisation [1569]. A study from Indiana showed that spina bifida patients who transitioned tended to have more active health issues and more radiographic tests prior to discharge, and were less likely to use emergency department services, although there remained a significant issue with outpatient attendance compliance [1570]. However, a subsequent study from Oklahoma found that those who participated in a transition clinic were more successful in transferring from paediatric to adult care, with improved subsequent clinic attendances, and that early introduction to adult providers as well as an increased number of visits positively impacted compliance [1571]. It has been shown that transition readiness can be improved with clinic experience, and the relationship with the paediatric urologist can further facilitate this process [1572]. Overall, successful transition of spina bifida patients results in a relative decrease in unplanned hospital admissions, unplanned outpatient clinic attendances, and preventable emergency department visits [1573].
27.4.2. Posterior urethral valves
Despite early intervention, many posterior urethral valves (PUV) patients have inherently abnormal bladders. The ‘valve bladder’ is a progressive condition that continues to evolve over years, despite surgically alleviated bladder outlet obstruction during infancy. Clinically, this can present as urinary incontinence or polyuria, due to poor bladder compliance, detrusor overactivity, VUR, ureterovesical junction obstruction or myogenic failure [1547,1574]. It is essential to the adult urologist to recognise risk factors (dilatation of upper urinary tract, progressive loss of renal function, detrusor non-compliance) for progressive lower urinary tract dysfunction in adult men with PUV. Life-long monitoring, including serial renal function blood tests, upper tract imaging and urodynamic studies, has been advocated [1574]. Treatment options, analogous to neurogenic bladder patients, are tailored to the specific patient and includes behavioural modifications, nocturnal bladder emptying, pelvic floor muscle therapy, anticholinergics, CIC, alpha antagonist, and in selected cases, bladder augmentation [1574].
Chronic kidney disease develops in up to 32% of PUV patients and approximately 20% of these progress towards ESRD [1231]. Renal transplantation in these patients can be performed safely and effectively [1299,1300]. Prior to transplantation, a full bladder and voiding assessment is recommended. Renal function should be monitored throughout life by both an adult urologist and a nephrologist [1547,1574] (see Chapter 21 on congenital lower urinary tract obstruction).
27.4.3. Hypospadias
Hypospadias is usually diagnosed and treated in early childhood. Being a dynamic condition, hypospadias and its surgical approaches to repair tend to pose continuing challenges with time. Appropriate long-term follow-up remains controversial, because most patients with hypospadias do well with minimal further urologic issues after initial repair [1548]. Penile development, especially during puberty, can result in new functional concerns. Additionally, some complications, including fertility, sexual dysfunction and cosmetic dissatisfaction, only become apparent as patients became sexually active [1547,1575]. In adult hypospadias patients with urological issues, urethral strictures and lower urinary tract symptoms (45-72% and 50-82%, respectively) are the most commonly presenting conditions. This is followed by urethrocutaneous fistula (16-30%), uncorrected hypospadias (14-43%), spraying of the urinary stream (24%), UTI (15-25%), ventral curvature (14-24%), lichen sclerosus (8-43%), dysuria (10%), and general genital dissatisfaction [1575]. It is recommended that adult patients are, therefore, best addressed by a urethral reconstructive urologist, as a general urologist may have limited exposure to the complex urethral reconstructive procedures often required to address these issues [1547].
To lessen the difficulties in transitioning hypospadias patients from a paediatric to an adult urologist, follow-up throughout childhood and adolescence is advisable [1575]. Furthermore, it may be prudent to educate adolescent patients to enable them to take ownership of their condition and an awareness of prior surgical management (see Chapter 9 on hypospadias).
27.4.4. Bladder-exstrophy-epispadias complex
The management of bladder exstrophy-epispadias complex (BEEC) in infants is well-established, and continence outcomes in specialist centres are well-described [1576]. On the contrary, adolescent and adult care is rarely formally centralised, even though similar complex challenges exist [1545]. Children with cloacal or bladder exstrophy may require bladder augmentation or diversion with closure of the bladder neck and the creation of a catheterisable channel. These children are at risk of long-term complications associated with the interposition of bowel segments into the bladder [1547,1576]. In addition to urinary function, sexual and reproductive function can be impaired for both sexes. In men, dorsal penile curvature, a reduced corporal volume and a widened pubic symphysis can result in a short functional penile length. Men with epispadias can also experience difficulties with retrograde ejaculation. In women, vaginal stenosis (31%) and pelvic organ prolapse may be present. Pregnancy is possible but with an increased risk of preterm labour. Scheduling these patients for an elective caesarean section should be considered to avoid potential complications associated with spontaneous vaginal delivery [1545,1547,1548,1577].
Individuals with BEEC are at an increased risk of developing cancer, with the majority being diagnosed at a younger age compared to the general population and typically presenting with nonurothelial types [1576,1578,1579]. A systematic review indicated that 56% of BEEC patients with cancer are diagnosed between the ages of 45 and 67, while 37% are diagnosed between 0 and 44 years of age. The male-to-female ratio among these patients is 2.7:1, and adenocarcinoma accounts for 68% of the tumour types identified [1578]. Although screening for symptoms of urothelial cancers in individuals with BEEC has been suggested, no standardised surveillance protocols have been established to date [1576,1578].
Due to the complexity involved in the management of the paediatric BEEC patient, a similar transitional approach and infrastructure is recommended for this cohort who transition to adult care [1577].
27.4.5. Differences of sex development
Differences of sex development (DSD) encompass a broad spectrum of diagnoses, of which the majority of individuals present with ambiguous genitalia at or shortly after birth and are cared for by paediatric services throughout childhood. However, a proportion of children with DSD present in early adolescence and spend only a short time in paediatric care before transition to adult services.
During transition, a general move towards independence and self-responsibility is pertinent, as is a more specific focus on discussing the DSD diagnosis with the individuals themselves, along with the details of any treatment history and potential further management as the individuals mature [1580,1581]. Studies of children with congenital adrenal hyperplasia (CAH) have shown that providing the adolescent with knowledge regarding the pathophysiology of CAH, an understanding of their medication regimen, skills to self-manage stress-dose steroids during illness, knowledge of sexual function, and fertility expectations has empowered these children to take primary responsibility for their care and transition into adulthood [1582]. It has also been shown that transition readiness is higher among CAH adolescents with good medication-adherence rates [1583]. Transitional care for children with DSD requires continuity of an expert multidisciplinary team, supporting the child and their families in an environment comprising specialists (endocrinology, surgery, urology, psychology/psychiatry, gynaecology, genetics, social work and nursing) with experience from both paediatric and adult practice (See Chapter 20 on disorders/difference of sex development).
27.5. Summary of evidence and recommendations for transitional urology
| Summary of evidence | LE |
| There are several paediatric urological conditions requiring long-term follow-up that would be unfamiliar to solely adult-trained urologists. | 4 |
| Involvement of paediatric and adult urologists working in a multidisciplinary team with expertise in the management and treatment of congenital conditions is essential. | 4 |
| Assessment of readiness may be formalised using readiness assessment questionnaires completed by both the child and caregivers to provide insight into their ability to cope with the transfer process and, therefore, represents a way of determining when the right time is for them to transition to adult services. | 4 |
| A gradual introduction of the adult urologist into the health care team, several years before targeted time of transition, may facilitate the transition. | 4 |
| Recommendations | Strength rating |
| Develop a standardised transition-of-care program and collaborate with adult providers to facilitate safe, successful and sustainable transition. | Strong |
| Start transition at the onset of adolescence involving both paediatric and adult urology providers in a multidisciplinary approach to ensure better transition readiness and subsequent adult clinic adherence. | Weak |
| Use a validated transition assessment tool to objectively assess for transition readiness. | Strong |