
16. DILATATION OF THE UPPER URINARY TRACT (PUJ OBSTRUCTION)
16.1. Epidemiology, aetiology and pathophysiology
Dilatation of the upper urinary tract (UUT) remains a significant clinical challenge in deciding which patient will benefit from treatment. Pelviureteric junction (PUJ) obstruction is defined as impaired urine flow from the pelvis into the proximal ureter, with subsequent dilatation of the collecting system and the potential to damage the kidney. PUJ obstruction is the most common pathological cause of neonatal hydronephrosis [790]. PUJ obstruction appears to have a multifactorial developmental origin, with intrinsic factors such as reduced density of Cajal-like cells and differential gene expression patterns affecting hypoxia, fibrosis, inflammation and neuronal regulation, in addition to extrinsic factors [791,792]. PUJ obstruction has an overall incidence of 1:1,500 and a ratio of males to females of 2:1 in newborns. PUJ obstruction is more common in males, and male sex is associated with a more-severe clinical course and a higher risk of reoperation compared to females [793,794]. It is more frequent on the left side. In children with severe hydronephrosis, higher mean systolic and diastolic blood pressures may be observed compared to controls, along with elevated active renin and aldosterone concentrations, with postoperative normalisation of blood pressure following pyeloplasty but persistent elevations in renin and aldosterone levels [795].
Defining ‘obstruction’ can be very difficult, as there is no clear division between ‘obstructed’ and ‘non-obstructed’ urinary tracts. Currently, the most popular definition is that an obstruction represents any restriction to urinary outflow that, if left untreated, will cause progressive renal deterioration [796].
16.2. Diagnostic evaluation
The widespread use of US during pregnancy has resulted in a higher detection rate for antenatal hydronephrosis [797]. The challenge in the management of dilated UUT is to decide which child should be observed, which should be managed medically, and which requires surgical intervention. Despite the wide range of diagnostic tests, there is no single test that can accurately distinguish obstructive from nonobstructive cases (see Figure 10).
16.2.1. Antenatal ultrasound
The kidneys are visualised routinely, usually between the 16th and 18th weeks of pregnancy, when almost all amniotic fluid consists of urine. The most sensitive time for foetal urinary tract evaluation is the 28th week. If dilatation is detected, US should focus on:
- laterality, severity of dilatation, and echogenicity of the kidneys;
- hydronephrosis or hydroureteronephrosis;
- bladder volume and bladder emptying;
- sex of the child; and
- amniotic fluid volume [798].
16.2.2. Postnatal ultrasound
Since transitory neonatal dehydration lasts approximately 48 hours after birth, imaging should be performed following this period of postnatal oliguria. However, in severe cases (bilateral dilatation, solitary kidney, oligohydramnios), immediate postnatal sonography is recommended [799]. Renal and bladder ultrasound (RBUS) should assess the anteroposterior diameter of the renal pelvis, calyceal dilatation, kidney size, thickness of the parenchyma, cortical echogenicity, ureters, bladder wall and residual urine.
16.2.3. Voiding cystourethrogram
In newborns with identified UUT dilatation, the primary or important associated factors that must be detected include:
- vesicoureteral reflux (found in up to 25% of affected children) [800];
- urethral valves;
- ureteroceles;
- diverticula; and
- neurogenic bladder.
Conventional voiding cystourethrogram (VCUG) is the method of choice for primary diagnostic procedures [801]. A VCUG is not normally considered necessary in unilateral hydronephrosis in the absence of ureteral dilatation and bladder abnormalities in RBUS performed with adequate bladder filling. VCUG should be considered in patients with urinary tract infection, ureteral dilatation or bladder abnormality, and bilateral hydronephrosis in males [802-805]. The objective in these instances is to exclude VUR, obstruction and obstructive pathologies. The routine use of VCUG prior to pyeloplasty does not impact surgical outcomes [805] and should therefore be used selectively.
16.2.4. Diuretic renography
Diuretic renography is the most commonly used diagnostic tool to detect the severity and functional significance of problems with urine transport. Technetium-99m (99mTc) mercaptoacetyltriglycine (MAG3) is the radionuclide of choice. It is important to perform the study under standardised circumstances (hydration, transurethral catheter) after the fourth and sixth weeks of life [806]. Oral fluid intake is encouraged prior to the examination. At fifteen minutes before the injection of the radionuclide, it is mandatory to administer normal saline intravenous infusion at a rate of 15mL/kg over 30 minutes, with a subsequent maintenance rate of 4mL/kg/h throughout the entire period of the investigation [807]. The recommended dose of furosemide is 1mg/kg for infants during the first year of life, while 0.5mg/kg should be given to children aged one to sixteen years, up to a maximum dose of 40mg.
Beyond evaluating drainage curves, prolonged T½ drainage times have been associated with a higher likelihood of requiring surgical intervention [808]. Functional magnetic resonance urography (fMRU) is a radiation-free alternative providing detailed anatomical and functional information comparable to MAG3 renography, although its clinical use remains limited [809].
16.2.5. Severity classification and risk stratification
Severity of upper urinary tract dilatation is assessed using a combination of ultrasonographic findings and functional parameters. Classification systems such as the Society for Fetal Urology (SFU) grading, anteroposterior pelvic diameter (APD) measurement, and the Urinary Tract Dilation (UTD) classification help stratify risk for intervention [810-812]. No single system has been shown to be superior and universally adopted [813]. Clinical practice typically relies on integrating multiple ultrasonographic features, including calyceal dilation, parenchymal thickness, ureteral abnormalities and bladder findings, along with the assessment of drainage and renal function. Given the long-term risk of renal injury associated with UTD P2 and P3, ongoing clinical follow-up through childhood is recommended [810,814].
16.2.6. Biomarkers
Currently, urinary biomarkers may complement but cannot replace conventional imaging in the diagnostic workup of UUT dilatation. Urinary biomarkers have been evaluated as adjuncts to imaging in children with antenatal hydronephrosis and suspected obstruction. Meta-analyses and systematic reviews suggest that markers such as neutrophil gelatinase-associated lipocalin (NGAL), kidney injury molecule-1 (KIM-1), and carbohydrate antigen 19-9 (CA19-9) may differentiate obstructive from nonobstructive dilatation and predict surgical need [815,816]. Urinary NGAL, monocyte chemoattractant protein-1 (MCP-1), interleukin-6 (IL-6), and CA19-9 have shown associations with obstruction severity [817-820].
Combinations of markers, such as MMP-7 with TIMP-2, or biomarker panels integrated with ultrasound parameters, have further improved diagnostic accuracy [821,822]. Although reported performance is promising, with areas under the curve of 0.80-0.90, methodological heterogeneity, limited cohort sizes, and lack of external validation preclude routine clinical application [815,823,824]. Moreover, these biomarkers are not universally available and not used in daily clinical practice.
Figure 10: Diagnostic algorithm for dilatation of the upper urinary tract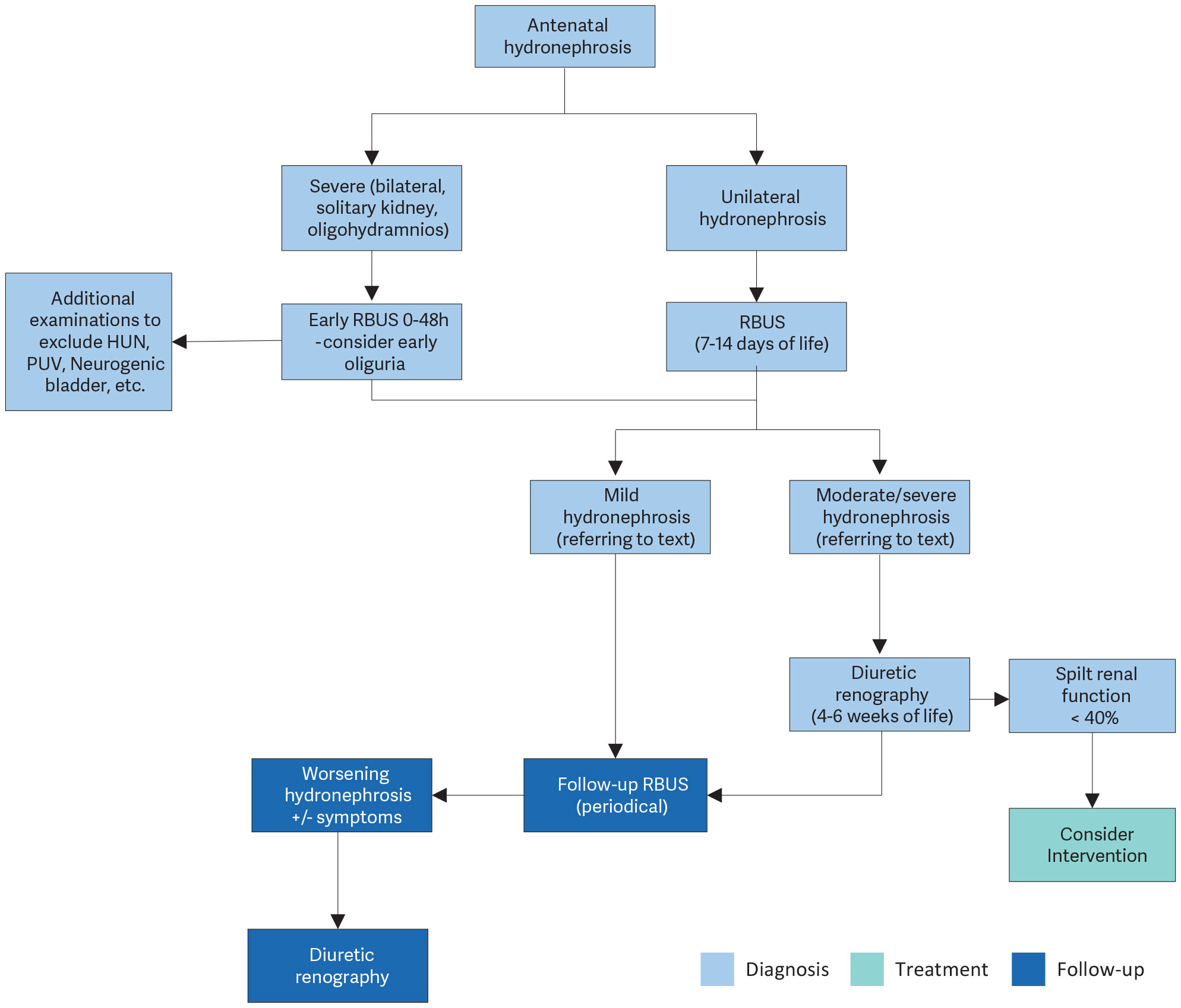 HUN = hydroureteronephrosis; PUV = posterior urethral valves; RBUS = renal, bladder ultrasound.
HUN = hydroureteronephrosis; PUV = posterior urethral valves; RBUS = renal, bladder ultrasound.16.3. Management
16.3.1. Prenatal management
Counselling the caregivers of an affected child is one of the most important aspects of care. The prognosis is hopeful for a hydronephrotic kidney, even if it is severely affected, because it may still be capable of meaningful renal function, unlike a severely hypoplastic and dysplastic kidney.
16.3.1.a. Continuous antibiotic prophylaxis
The benefits and harms of continuous antibiotic prophylaxis (CAP) versus observation in patients with hydronephrosis are controversial. Currently, most evidence for CAP is generally based on infants with antenatal hydronephrosis (ANH) involving various etiologies. CAP is not recommended for asymptomatic PUJ obstruction.
The Panel conducted a systematic review assessing the literature from 1980 onwards [825]. The key findings are summarised below.
Due to the heterogeneity of the published literature, no strong conclusions could be drawn as to whether CAP is superior to observation alone in children diagnosed with ANH involving various etiologies (hydronephrosis [HN], hydroureteronephrosis [HUN], vesicoureteral reflux [VUR] and so on). However, the evidence in the form of prospective and retrospective observational studies has shown that CAP reduces the risk of UTI in particular subgroups. Uncircumcised infants, HUN and high-grade HN may be more likely to develop UTI. CAP can be reserved for this subgroup of patients who are proven to be a high risk [825]. The SR was unable to identify the most effective antibiotic regime and present data on adverse effects. The most commonly chosen antibiotic in infants with ANH was trimethoprim.
16.3.2. PUJ obstruction
Management decisions must be made based on serial investigations that have used the same technique and have been performed by the same institution under standardised circumstances. Nevertheless, as the current available diagnostic tools are imprecise to some degree, indications for surgery are often amassed retrospectively and at the cost of losing irrevocably valuable renal function. According to a Cochrane review, nonsurgical management of unilateral PUJ obstruction in infants less than two years old is an option. However, the high risk of bias of the included studies limits the evidence of this systematic review [826]. In symptomatic cases (recurrent flank pain, febrile UTI), surgical correction is warranted. Additionally, surgical intervention is recommended in the event of impaired split renal function (< 40%), a decrease of split renal function of > 10% points in subsequent studies, poor drainage function after the administration of furosemide, increased anteroposterior diameter on US, and grade III and IV dilatation [827,828] as defined by the Society for Fetal Urology [829]. Supranormal differential renal function (≥ 55%) has been observed in approximately 15% of children with suspected PUJ obstruction [830,831]. However, current evidence suggests that supranormal function alone is not predictive of an increased need for surgical intervention [830,831], and decisions should remain based on anatomical severity, drainage assessment and clinical symptoms.
Management of PUJ obstruction in poorly functioning kidneys (arbitrarily defined as < 20% differential function) is controversial. The chance of function improvement appears limited, so a staged approach after a trial of temporary diversion does not seem advantageous and only increase treatment burden. The options of primary pyeloplasty or nephrectomy should be discussed with the family. In addition, conservative management can be considered in some patients, but no evidence-based and shared criteria are available to date to select out these patients. Multiple parameters in addition to split function can help in the decision-making, including patient age, symptoms, degree of the dilatation, parenchymal appearance and parent preferences. While some evidence suggests that pyeloplasty may lead to improvement in DRF even in poorly functioning kidneys [832-835], interpretation is constrained by the inherent variability of DRF measurement itself, where changes may reflect methodological margin of error rather than true functional gain.
Dismembered pyeloplasty, as described by Hynes and Anderson [836], is widely recognised as the gold standard for surgical correction of PUJ obstruction, with a reported success rate of approximately 95% [822,837-839]. Regardless of the surgical approach - open pyeloplasty (OP) or minimally invasive surgery (MIS), including laparoscopic pyeloplasty (LP) and robot-assisted laparoscopic pyeloplasty (RALP) - comparable success and complication rates have been reported [837-839]. Established advantages of MIS over OP include shorter length of hospital stays, improved cosmetic outcomes, less postoperative pain and early recovery [837,839].
MIS in infants (≤ 1 year of age) has demonstrated comparable perioperative outcomes and similar success rates to OP, with longer operative times [822,840].
16.4. Summary of evidence and recommendations for the management of PUJ obstruction
Summary of evidence | LE |
Nowadays, most hydronephrotic kidneys have already been diagnosed prenatally during a maternal US investigation. | 2 |
Pelviureteric junction (PUJ) obstruction is the leading pathological cause of hydronephrotic kidneys. | 1 |
In children diagnosed with antenatal hydronephrosis, a systematic review could not establish any benefits or harms related to continuous antibiotic prophylaxis. | 1b |
In children diagnosed with antenatal hydronephrosis, uncircumcised infants, children diagnosed with high-grade hydronephrosis and hydroureteronephrosis were shown to be at higher risk of developing UTI. | 2 |
Recommendations | Strength rating |
Include serial ultrasound (US) and subsequent diuretic renogram and sometimes voiding cystourethrography in postnatal investigations. | Strong |
Offer continuous antibiotic prophylaxis to the subgroup of children with antenatal hydronephrosis who are at high risk of developing urinary tract infection such as uncircumcised infants, children diagnosed with hydroureteronephrosis and high-grade hydronephrosis, respectively. | Weak |
Decide on surgical intervention based on the time course of the hydronephrosis and the impairment of renal function. | Weak |
Offer surgical intervention in case of an impaired split renal function due to obstruction or a decrease of split renal function in subsequent studies and increased anteroposterior diameter on the US, and grade IV dilatation as defined by the Society for Fetal Urology. | Weak |
Offer pyeloplasty when ureteropelvic junction obstruction has been confirmed clinically or with serial imaging studies proving a substantially impaired or decrease in function. | Weak |