
23. EMERGENCIES IN PAEDIATRIC UROLOGY
23.1. Acute scrotum
Refer to Chapter 8 on acute scrotum.
23.2. Paraphimosis
Refer to Chapter 3 on phimosis and other abnormalities of the penile skin.
23.3. Priapism
23.3.1. Epidemiology, aetiology and pathophysiology
Priapism is a prolonged full or partial erection of the penis unrelated to sexual stimuli lasting ≥ 4 hours. Although the prevalence of priapism in children is not well-reported in literature, it is considered a rare disease. The most common cause of priapism in children is sickle cell disease (SCD), which accounts for approximately 65% of all cases, followed by leukaemia (10%), trauma (10%), idiopathic (10%) and drugs (5%) [1405]. In patients with SCD, the mean age of the first episode of priapism has been shown to be 15 years old, with 25% presenting prepubertally [1406].
23.3.2. Classification
Priapism in children can be divided in four groups: ischaemic (low-flow) priapism, stuttering priapism, nonischaemic (high-flow) priapism, and neonatal priapism.
Ischaemic (low-flow, veno-occlusive) priapism is the most common form (95%) in children. It presents as a painful, rigid erection, with decreased or absent intracavernous arterial inflow. This is considered a medical emergency, since a duration of ≥ 4 hours can cause ischaemia within the corpora cavernosa, and eventually irreversible damage, such as smooth muscle necrosis, corporal fibrosis and erectile dysfunction [1407].
Stuttering priapism presents as recurrent, self-limiting, prolonged erections, with intervening periods of detumescence. This often precedes an episode of ischaemic (low-flow) priapism [1408].
Non-ischaemic (high-flow, arterial) priapism is a prolonged erection of the penis lasting ≥ 4 hours not associated with ischaemia. The most common cause is penile, perineal or pelvic trauma, which can lead to the development of an arteriolar-sinusoidal or arteriocavernous fistula, and usually has a delayed presentation after trauma (three hours to seven days) [1409].
Neonatal priapism is a very rare condition, with only a few case series described in literature. The conditions presents as a prolonged erection of the penis ≥ 4 hours in a newborn. Sickle cell disease is not associated with neonatal priapism, due to the presence of foetal haemoglobin. Neonatal priapism is most commonly idiopathic, but polycythaemia is the most common cause among the identifiable causes [1410]. It also has a favourable natural history and benign pathophysiology.
23.3.3. Diagnostic evaluation
History
A comprehensive history is critical in priapism and can determine the underlying priapism subtype and cause. Table 8 presents key points in the history of a child with priapism.
Table 8: Key points in the history for a child with priapism (adapted from Broderick et al. [1411])
| Key points in the history for a child with priapism |
| Duration of erection |
| Presence and severity of pain |
| Previous episodes of priapism and methods of treatment |
| Medications or recreational drug use |
| Sickle cell disease, haemoglobinopathies, hypercoagulable states, vasculitis |
| Trauma to the pelvis, perineum or penis |
Physical examination
Inspection and palpation of the penis is recommended to assess the degree of tumescence and rigidity and the involvement of the corpora cavernosa, spongiosum and glans. In ischaemic (low-flow) priapism, typically the glans and corpus spongiosum are flaccid. In nonischaemic (high-flow) priapism, typically the corpora and the glans are tumescent, but not fully rigid (Table 9). If perineal compression results in detumescence, this is suggestive of a non-ischaemic (high-flow) priapism.
Penile imaging
Colour doppler ultrasonography of the penis and perineum should be performed in all patients. This can support clinical differentiation between ischaemic (low-flow) and nonischaemic (high-flow) priapism with 100% sensitivity and 73% specificity in adults [1412], where a peak systolic velocity < 50cm/s and a mean velocity < 6.5cm/s are suspicious for ischaemia [1413].
Laboratory testing
Laboratory testing with complete blood count (white blood cell count with blood cell differential platelet count) and specific tests for SCD or other haemoglobinopathies should be performed. When ischaemic (low-flow) priapism is suspected, penile blood gas analysis should be performed to differentiate between ischaemic (low-flow) and non-ischaemic (high-flow) priapism (Table 10). However, when non-ischaemic (high-flow) priapism is suspected, penile blood gas analysis should not be the diagnostic of first choice, due to the invasive nature and need for anaesthesia.
Table 9: Key findings in paediatric priapism (adapted from Donaldson et al., and Broderick et al. [1405,1411])
| Ischaemic (low-flow) priapism | Non-ischaemic (high-flow) priapism | |
| Corpora cavernosa fully rigid | Typically | Seldom |
| Penile pain | Typically | Seldom |
| History of stuttering priapism | Typically | Seldom |
| Haematological abnormalities | Typically | Seldom |
| Abnormal penile blood gas | Typically | Seldom |
| Perineal trauma | Seldom | Typically |
Table 10: Blood gas analysis (adapted from Broderick et al. [1411])
| Source | pO2 (mmHg) | pCO2 (mmHg) | pH |
| Normal arterial blood (room air) (similar values are found in nonischaemic priapism) | > 90 | < 40 | 7.40 |
| Normal mixed venous blood (room air) | 40 | 50 | 7.35 |
| Ischaemic priapism (first corporal aspirate) | < 30 | > 60 | < 7.25 |
23.3.4. Disease management
Differentiation between ischaemic (low-flow) and non-ischaemic (high-flow) priapism is essential since clinical management differs between the two. Ischaemic (low-flow) priapism is a medical emergency requiring immediate treatment, where non-ischaemic (high-flow) priapism does not. The management of a child with ischaemic (low-flow) priapism is in most parts similar to adults [1414].
Ischaemic (low-flow) priapism
Conservative
Although the amount of evidence is low, conservative treatment should be advised (e.g. physical exercise, urination, cold bath, ejaculation, oral/IV fluids and analgesia), however, if symptoms persist ≥ 2 hours, urgent medical care should be sought [1415].
Medical
If conservative treatment fails, a step-up approach should be used for the management of priapism [1405]. Firstly, anaesthesia should be given for the child - either local anaesthesia, dissociative sedation or general anaesthesia, depending on the availability of paediatric anaesthetic expertise and the age and condition of the child. In SCD, there are increased risks for general anaesthesia that should be taken into account [1416]. Subsequently, a step-up approach should be used for treatment (Figure 15), adapted from Donaldson and the adult priapism guideline [1405,1414].
Figure 15: Step-up approach for the management of Ischaemic (low-flow) priapism in children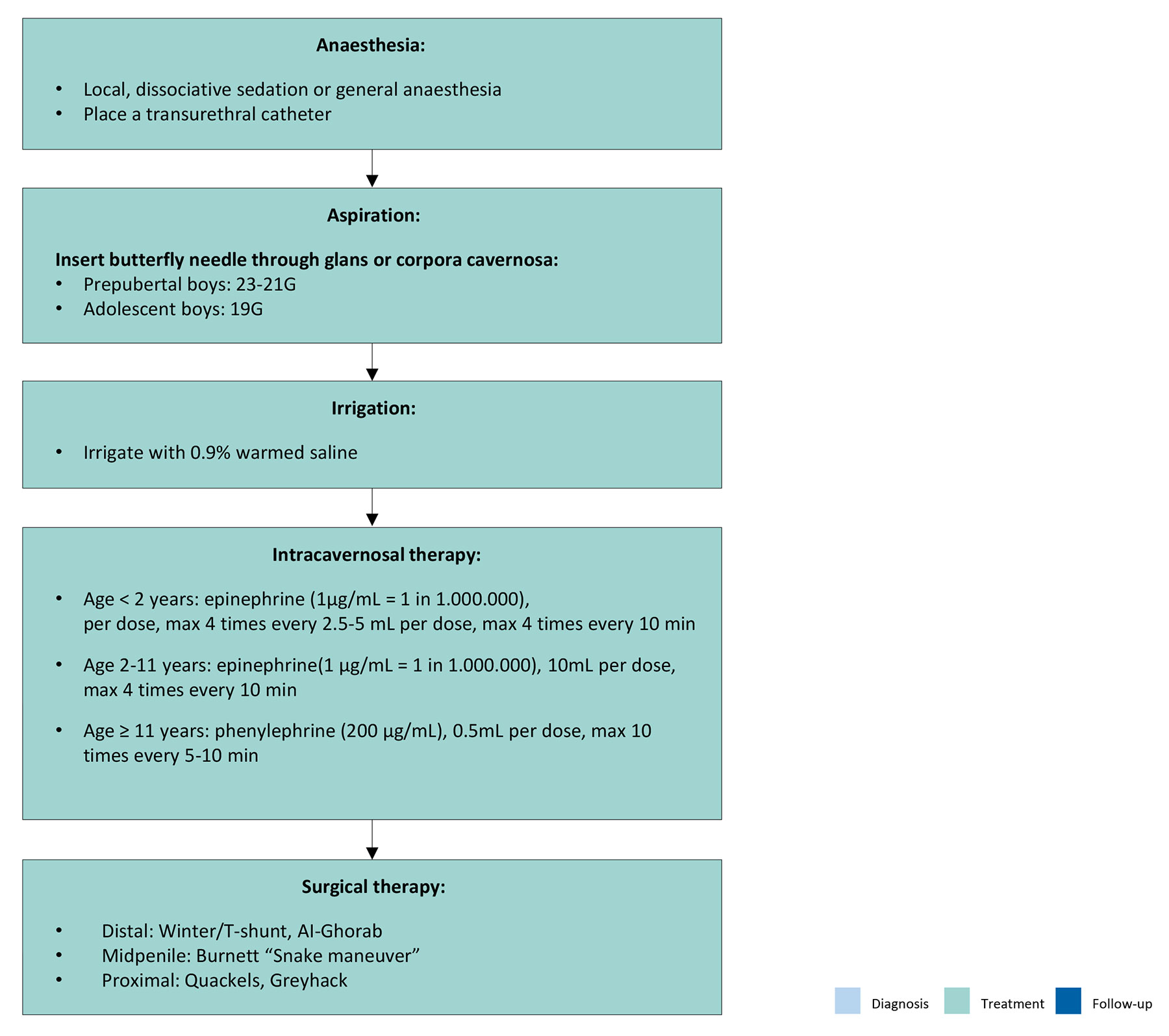
Nonischaemic (high-flow) priapism
Nonischaemic (high-flow) priapism is a very rare entity in the paediatric population. The treatment of nonischaemic (high-flow) priapism is not emergent. One study demonstrated that conservative management and long-term follow-up yielded no evidence of erectile dysfunction after a median follow-up of 55 months [1417]. Conservative treatment, such as perineal compression or application of ice to the perineum, can be successful. If symptoms persist, super-selective angioembolisation can be performed, however, this is technically challenging in children and requires a specialist paediatric vascular radiologist [1418]. Children should be initially treated with conservative management, reserving embolisation for refractory cases [1419].
Stuttering priapism, and priapism associated with sickle cell disease (SCD)
The management of a prolonged erection in stuttering priapism is similar to ischaemic (low-flow) priapism. Further management should focus on the prevention of further episodes. Several agents are proposed in literature, such as α-adrenergic agonists, PDE-5 inhibitors, hydroxyurea, β-agonists or gonadotropin-releasing hormone agonists, but evidence is limited.
The acute management of SCD priapism is closely related to that outlined above. The main caveat is that those with SCD should have their disease medically optimised in close conjunction with paediatric haematology/oncology through a multidisciplinary approach. Hydroxyurea may decrease crisis frequency and severity in SCD-associated priapism [1420]. Unlike urgent surgical management performed in the adult population, a minimally invasive management strategy can be implemented in the paediatric population, where an extended period of conservative management that avoids operative management under general anaesthetic can be effective in approximately 60% cases [1421].
Neonatal priapism
Neonatal priapism is usually self-limiting and rarely requires treatment. Careful observation is appropriate in most cases since the majority resolve spontaneously without sequelae. If underlying polycythaemia is present, this could be treated by venesection and fluid resuscitation [1422].
23.4. Summary of evidence and recommendations for the diagnosis and management of priapism
| Summary of evidence | LE |
| The most common cause of priapism in children is sickle cell disease. | 3 |
| Ischaemic (low-flow, veno-occlusive) priapism is the most common form (95%) in children and is considered a medical emergency. | 3 |
| Colour doppler ultrasonography of the penis and perineum can support clinical differentiation between ischaemic (low-flow) and nonischaemic (high-flow) priapism in children. | 2b |
| Recommendations | Strength rating |
| Perform a doppler ultrasonography in all patients presenting with priapism. | Strong |
| In children with ischaemic (low-flow) priapism, perform a full blood count and haemoglobinopathy screen to exclude sickle cell disease or other haematological disorders. | Strong |
| Adopt a multidisciplinary approach when managing patients with SCD-associated priapism. | Strong |
| Use a stepwise approach starting with the least invasive therapy in patients with ischaemic (low-flow) priapism. | Strong |
| Manage neonatal and non-ischaemic (high-flow) priapism conservatively in the initial management period. | Strong |